

Phase I study of safety and immunogenicity of an Escherichia coli-derived recombinant protective antigen (rPA) vaccine to prevent anthrax in adults
- PMID: 21079762
- PMCID: PMC2974626
- DOI: 10.1371/journal.pone.0013849
Phase I study of safety and immunogenicity of an Escherichia coli-derived recombinant protective antigen (rPA) vaccine to prevent anthrax in adults
Abstract
Background: The fatal disease caused by Bacillus anthracis is preventable with a prophylactic vaccine. The currently available anthrax vaccine requires a lengthy immunization schedule, and simpler and more immunogenic options for protection against anthrax are a priority for development. In this report we describe a phase I clinical trial testing the safety and immunogenicity of an anthrax vaccine using recombinant Escherichia coli-derived, B. anthracis protective antigen (rPA).
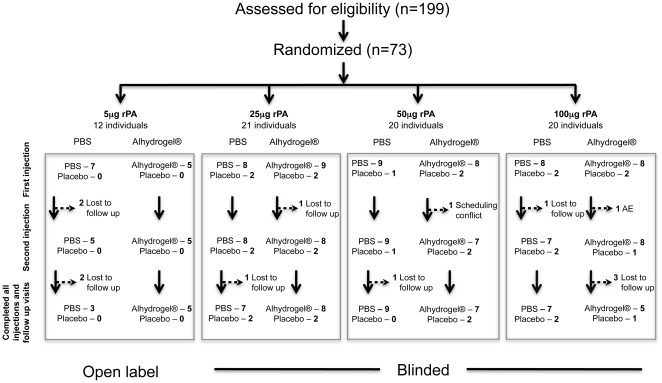
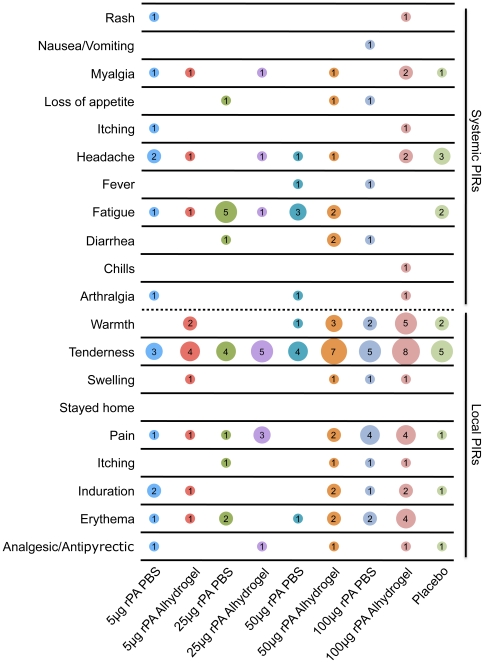
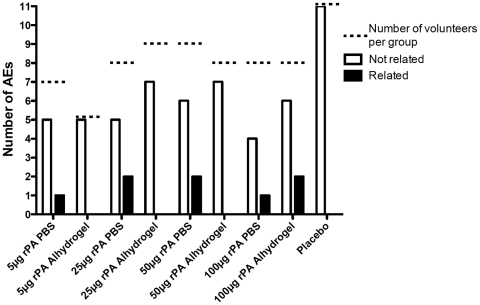
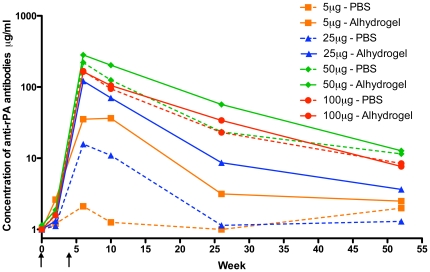
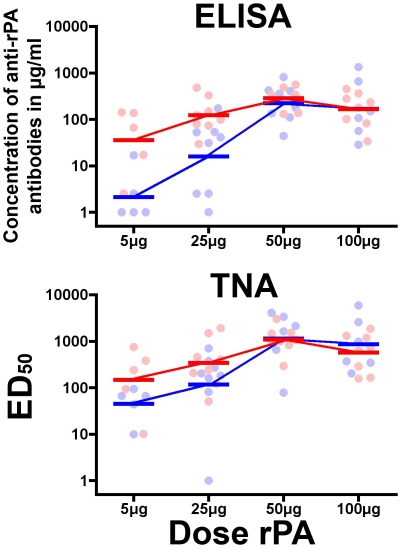
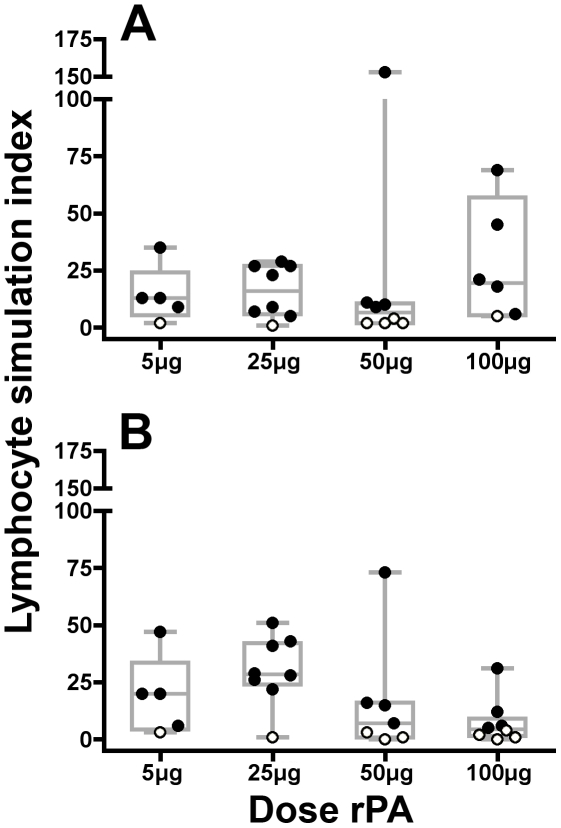
Methodology/principal findings: A total of 73 healthy adults ages 18-40 were enrolled and 67 received 2 injections separated by 4 weeks of either buffered saline placebo, or rPA formulated with or without 704 µg/ml Alhydrogel® adjuvant in increasing doses (5, 25, 50, 100 µg) of rPA. Participants were followed for one year and safety and immunologic data were assessed. Tenderness and warmth were the most common post-injection site reactions. No serious adverse events related to the vaccine were observed. The most robust humoral immune responses were observed in subjects receiving 50 µg of rPA formulated with Alhydrogel® with a geometric mean concentration of anti-rPA IgG antibodies of 283 µg/ml and a toxin neutralizing geometric 50% reciprocal geometric mean titer of 1061. The highest lymphoproliferative peak cellular response (median Lymphocyte Stimulation Index of 29) was observed in the group receiving 25 µg Alhydrogel®-formulated rPA.
Conclusions/significance: The vaccine was safe, well tolerated and stimulated a robust humoral and cellular response after two doses.
Trial registration: ClinicalTrials.gov NCT00057525.
Conflict of interest statement
Figures
References
-
- Young JA, Collier RJ. Anthrax toxin: receptor binding, internalization, pore formation, and translocation. Annu Rev Biochem. 2007;76:243–265. - PubMed
-
- Fellows PF, Linscott MK, Ivins BE, Pitt ML, Rossi CA, et al. Efficacy of a human anthrax vaccine in guinea pigs, rabbits, and rhesus macaques against challenge by Bacillus anthracis isolates of diverse geographical origin. Vaccine. 2001;19:3241–3247. - PubMed
-
- Ivins BE, Fellows PF, Pitt ML, Estep JE, Welkos SL, et al. Efficacy of a standard human anthrax vaccine against Bacillus anthracis aerosol spore challenge in rhesus macaques. Salisbury Med Bull. 1996;87:125–126.
-
- Ivins BE, Pitt ML, Fellows PF, Farchaus JW, Benner GE, et al. Comparative efficacy of experimental anthrax vaccine candidates against inhalation anthrax in rhesus macaques. Vaccine. 1998;16:1141–1148. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
