

Feasibility and safety of high-dose adenosine perfusion cardiovascular magnetic resonance
- PMID: 21080924
- PMCID: PMC2996376
- DOI: 10.1186/1532-429X-12-66
Feasibility and safety of high-dose adenosine perfusion cardiovascular magnetic resonance
Abstract
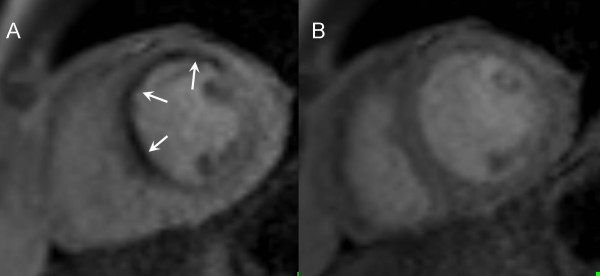
Introduction: Adenosine is the most widely used vasodilator stress agent for cardiovascular magnetic resonance (CMR) perfusion studies. With the standard dose of 140 mcg/kg/min some patients fail to demonstrate characteristic haemodynamic changes: a significant increase in heart rate (HR) and mild decrease in systolic blood pressure (SBP). Whether an increase in the rate of adenosine infusion would improve peripheral and, likely, coronary vasodilatation in those patients is unknown. The aim of the present study was to assess the tolerance and safety of a high-dose adenosine protocol in patients with inadequate haemodynamic response to the standard adenosine protocol when undergoing CMR perfusion imaging.
Methods: 98 consecutive patients with known or suspected coronary artery disease (CAD) underwent CMR perfusion imaging at 1.5 Tesla. Subjects were screened for contraindications to adenosine, and an electrocardiogram was performed prior to the scan. All patients initially received the standard adenosine protocol (140 mcg/kg/min for at least 3 minutes). If the haemodynamic response was inadequate (HR increase < 10 bpm or SBP decrease < 10 mmHg) then the infusion rate was increased up to a maximum of 210 mcg/kg/min (maximal infusion duration 7 minutes).
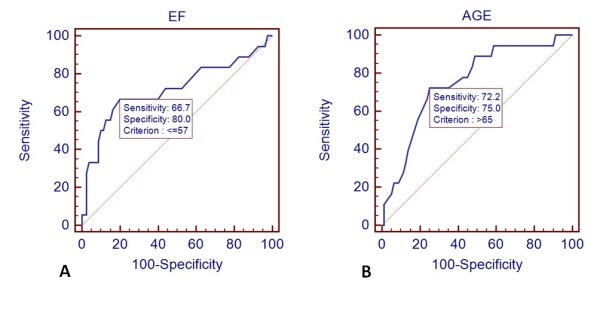
Results: All patients successfully completed the CMR scan. Of a total of 98 patients, 18 (18%) did not demonstrate evidence of a significant increase in HR or decrease in SBP under the standard adenosine infusion rate. Following the increase in the rate of infusion, 16 out of those 18 patients showed an adequate haemodynamic response. One patient of the standard infusion group and two patients of the high-dose group developed transient advanced AV block. Significantly more patients complained of chest pain in the high-dose group (61% vs. 29%, p = 0.009). On multivariate analysis, age > 65 years and ejection fraction < 57% were the only independent predictors of blunted haemodynamic responsiveness to adenosine.
Conclusions: A substantial number of patients do not show adequate peripheral haemodynamic response to standard-dose adenosine stress during perfusion CMR imaging. Age and reduced ejection fraction are predictors of inadequate response to standard dose adenosine. A high-dose adenosine protocol (up to 210 mcg/kg/min) is well tolerated and results in adequate haemodynamic response in nearly all patients.
Figures
Similar articles
-
Feasibility and safety of adenosine cardiovascular magnetic resonance in patients with MR conditional pacemaker systems at 1.5 Tesla.J Cardiovasc Magn Reson. 2015 Dec 22;17:112. doi: 10.1186/s12968-015-0218-x. J Cardiovasc Magn Reson. 2015. PMID: 26695427 Free PMC article.
-
A comparison of standard and high dose adenosine protocols in routine vasodilator stress cardiovascular magnetic resonance: dosage affects hyperaemic myocardial blood flow in patients with severe left ventricular systolic impairment.J Cardiovasc Magn Reson. 2021 Mar 18;23(1):37. doi: 10.1186/s12968-021-00714-7. J Cardiovasc Magn Reson. 2021. PMID: 33731141 Free PMC article.
-
Deactivation vs. asynchronous pacing - prospective evaluation of a protocol for rhythm management in patients with magnetic resonance conditional pacemakers undergoing adenosine stress cardiovascular magnetic resonance imaging.BMC Cardiovasc Disord. 2017 Jun 2;17(1):142. doi: 10.1186/s12872-017-0579-1. BMC Cardiovasc Disord. 2017. PMID: 28577544 Free PMC article.
-
Regadenoson in the detection of coronary artery disease.Vasc Health Risk Manag. 2008;4(2):337-40. doi: 10.2147/vhrm.s1798. Vasc Health Risk Manag. 2008. PMID: 18561509 Free PMC article. Review.
-
Aminophylline shortage and current recommendations for reversal of vasodilator stress: an ASNC information statement endorsed by SCMR.J Cardiovasc Magn Reson. 2018 Dec 20;20(1):87. doi: 10.1186/s12968-018-0510-7. J Cardiovasc Magn Reson. 2018. PMID: 30567577 Free PMC article. Review.
Cited by
-
Gadolinium-based Contrast Agents for Cardiac MRI: Use of Linear and Macrocyclic Agents with Associated Safety Profile from 154 779 European Patients.Radiol Cardiothorac Imaging. 2020 Oct 29;2(5):e200102. doi: 10.1148/ryct.2020200102. eCollection 2020 Oct. Radiol Cardiothorac Imaging. 2020. PMID: 33778622 Free PMC article.
-
Safety, feasibility, and hemodynamic response of regadenoson for stress perfusion CMR.Int J Cardiovasc Imaging. 2023 Sep;39(9):1765-1774. doi: 10.1007/s10554-023-02877-z. Epub 2023 Jun 24. Int J Cardiovasc Imaging. 2023. PMID: 37354385 Free PMC article.
-
Haemodynamic and hyperaemic effects of adenosine in patients with atrial fibrillation undergoing quantitative myocardial perfusion cardiovascular magnetic resonance.Eur Heart J Imaging Methods Pract. 2024 Dec 26;2(3):qyae127. doi: 10.1093/ehjimp/qyae127. eCollection 2024 Jul. Eur Heart J Imaging Methods Pract. 2024. PMID: 39726566 Free PMC article.
-
Safety and tolerability of regadenoson CMR.Eur Heart J Cardiovasc Imaging. 2014 Jul;15(7):753-60. doi: 10.1093/ehjci/jet278. Epub 2014 Jan 21. Eur Heart J Cardiovasc Imaging. 2014. PMID: 24451179 Free PMC article.
-
Prognostic Value of Quantitative Stress Perfusion Cardiac Magnetic Resonance.JACC Cardiovasc Imaging. 2018 May;11(5):686-694. doi: 10.1016/j.jcmg.2017.07.022. Epub 2017 Nov 15. JACC Cardiovasc Imaging. 2018. PMID: 29153572 Free PMC article.
References
-
- Christiansen JP, Karamitsos TD, Myerson SG, Francis JM, Neubauer S. Stress Perfusion Imaging Using Cardiovascular Magnetic Resonance: A Review. Heart Lung Circ. 2010. - PubMed
-
- Karamitsos TD, Arnold JR, Pegg TJ, Cheng AS, van Gaal WJ, Francis JM, Banning AP, Neubauer S, Selvanayagam JB. Tolerance and safety of adenosine stress perfusion cardiovascular magnetic resonance imaging in patients with severe coronary artery disease. Int J Cardiovasc Imaging. 2009;25:277–283. doi: 10.1007/s10554-008-9392-3. - DOI - PubMed
-
- Wilson RF, Wyche K, Christensen BV, Zimmer S, Laxson DD. Effects of adenosine on human coronary arterial circulation. Circulation. 1990;82:1595–1606. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
