

Acoustic cardiac triggering: a practical solution for synchronization and gating of cardiovascular magnetic resonance at 7 Tesla
- PMID: 21080933
- PMCID: PMC2998500
- DOI: 10.1186/1532-429X-12-67
Acoustic cardiac triggering: a practical solution for synchronization and gating of cardiovascular magnetic resonance at 7 Tesla
Abstract
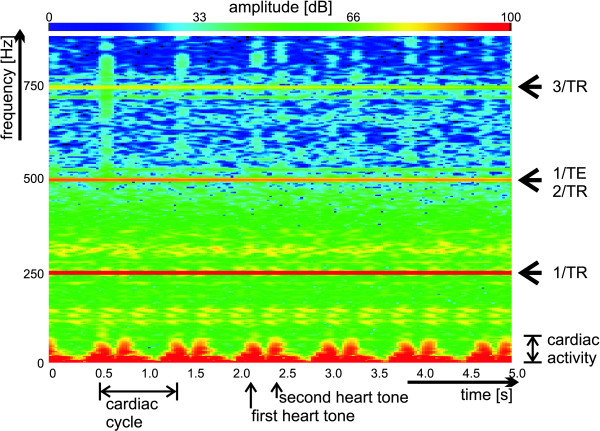
Background: To demonstrate the applicability of acoustic cardiac triggering (ACT) for imaging of the heart at ultrahigh magnetic fields (7.0 T) by comparing phonocardiogram, conventional vector electrocardiogram (ECG) and traditional pulse oximetry (POX) triggered 2D CINE acquisitions together with (i) a qualitative image quality analysis, (ii) an assessment of the left ventricular function parameter and (iii) an examination of trigger reliability and trigger detection variance derived from the signal waveforms.
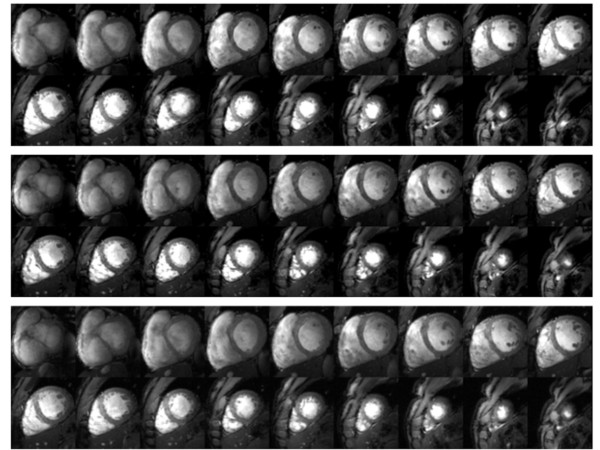
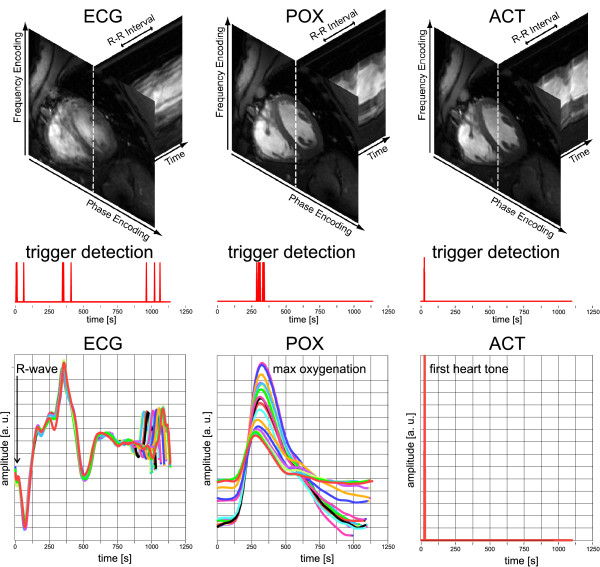
Results: ECG was susceptible to severe distortions at 7.0 T. POX and ACT provided waveforms free of interferences from electromagnetic fields or from magneto-hydrodynamic effects. Frequent R-wave mis-registration occurred in ECG-triggered acquisitions with a failure rate of up to 30% resulting in cardiac motion induced artifacts. ACT and POX triggering produced images free of cardiac motion artefacts. ECG showed a severe jitter in the R-wave detection. POX also showed a trigger jitter of approximately Δt = 72 ms which is equivalent to two cardiac phases. ACT showed a jitter of approximately Δt = 5 ms only. ECG waveforms revealed a standard deviation for the cardiac trigger offset larger than that observed for ACT or POX waveforms.Image quality assessment showed that ACT substantially improved image quality as compared to ECG (image quality score at end-diastole: ECG = 1.7 ± 0.5, ACT = 2.4 ± 0.5, p = 0.04) while the comparison between ECG vs. POX gated acquisitions showed no significant differences in image quality (image quality score: ECG = 1.7 ± 0.5, POX = 2.0 ± 0.5, p = 0.34).
Conclusions: The applicability of acoustic triggering for cardiac CINE imaging at 7.0 T was demonstrated. ACT's trigger reliability and fidelity are superior to that of ECG and POX. ACT promises to be beneficial for cardiovascular magnetic resonance at ultra-high field strengths including 7.0 T.
Figures




References
-
- Lanzer P, Botvinick EH, Schiller NB, Crooks LE, Arakawa M, Kaufman L, Davis PL, Herfkens R, Lipton MJ, Higgins CB. Cardiac imaging using gated magnetic resonance. Radiology. 1984;150:121–127. - PubMed
-
- Pattynama PM, van der Velde ET, Steendijk P, Lamb HJ, Baan J, de Roos A. Cardiovascular MR imaging: pressure-gating using the arterial pressure signal from a conventional ferromagnetic micromanometer-tip catheter. Magn Reson Imaging. 1994;12:531–534. doi: 10.1016/0730-725X(94)92547-X. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
