

Air encircling the intussusceptum on air enema for intussusception reduction: an indication for surgery?
- PMID: 21081577
- PMCID: PMC3473432
- DOI: 10.1259/bjr/19392930
Air encircling the intussusceptum on air enema for intussusception reduction: an indication for surgery?
Abstract
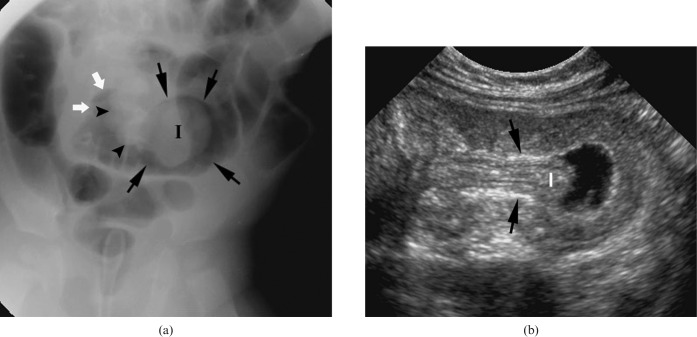
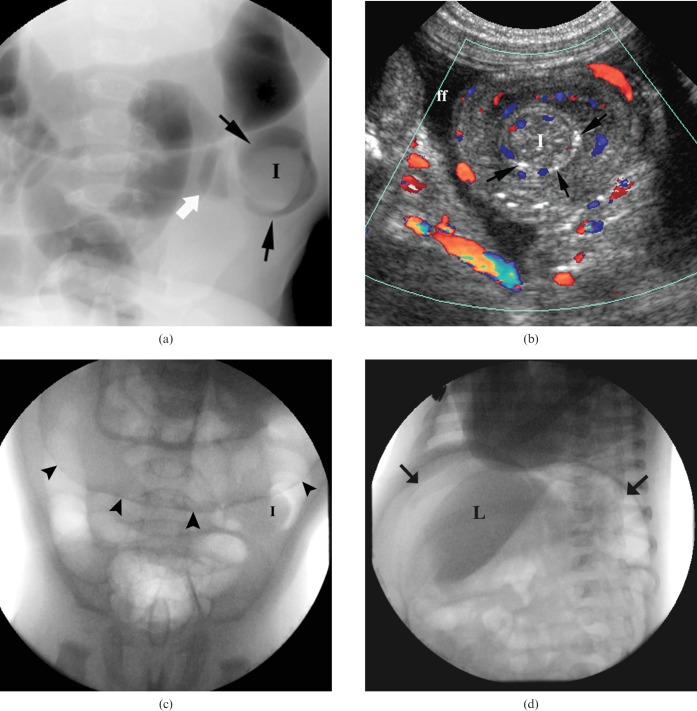
Objectives: The prompt identification of children in whom enema reduction of intussusception might fail and surgery is necessary is crucial in order to avoid futile repeat attempts and untoward complications. The purpose of this retrospective review was to determine whether air encircling the intussusceptum in the small bowel during air enema for intussusception reduction could serve as an indication for operation rather than repeat attempts at radiological reduction.
Methods: Imaging studies of 83 children aged 4 to 40 months with idiopathic intussusception who had air enema for intussusception reduction were reviewed for the presence of air encircling the intussusceptum in the distal small bowel. Findings were correlated with clinical course and surgical findings.
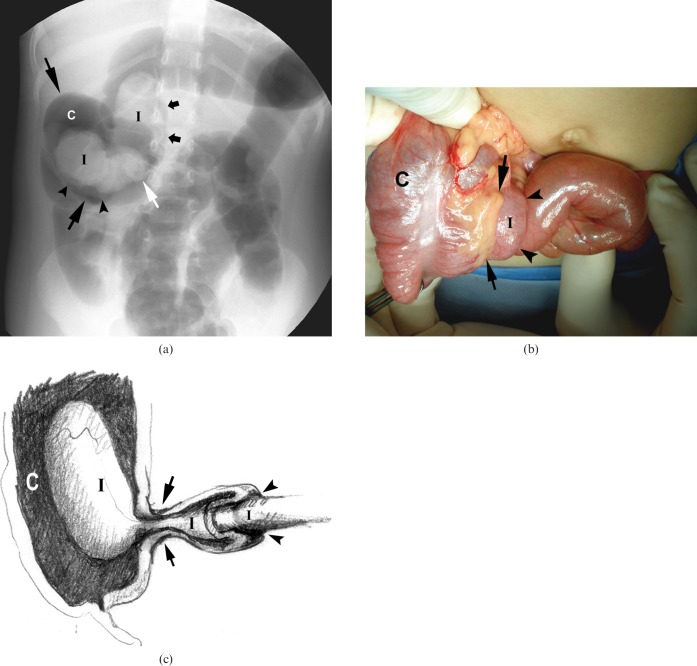
Results: In 12 of 83 patients, air was seen encircling the intussusceptum in the small bowel, and in 11 of these (88%) air enema failed to reduce the intussusception. In 8 of the 11, delayed repeated attempts using air enema failed to reduce intussusception. Clinical signs and their duration did not differ between those children without and those with air encircling the intussusceptum.
Conclusion: In the presence of air encircling the intussusceptum in the distal small bowel on air enema, delayed repeated attempts for intussusception reduction are unlikely to succeed, and surgery is indicated.
Figures

Similar articles
-
Delayed repeat enema in the management of intussusception.Pediatr Emerg Care. 2010 Sep;26(9):640-5. doi: 10.1097/PEC.0b013e3181ef0426. Pediatr Emerg Care. 2010. PMID: 20805784
-
Unsuccessful air-enema reduction of intussusception: is a second attempt worthwhile?Pediatr Surg Int. 1999;15(3-4):214-6. doi: 10.1007/s003830050558. Pediatr Surg Int. 1999. PMID: 10370026
-
Ultrasound features of intussusception predicting outcome of air enema.Pediatr Radiol. 1999 Sep;29(9):705-10. doi: 10.1007/s002470050679. Pediatr Radiol. 1999. PMID: 10460334
-
A large single-center experience in management of pediatric intussusception.Pediatr Int. 2023 Jan-Dec;65(1):e15495. doi: 10.1111/ped.15495. Pediatr Int. 2023. PMID: 36749147 Review.
-
Twenty years' experience for reduction of ileocolic intussusceptions by saline enema under sonography control.J Pediatr Surg. 2016 Jan;51(1):179-82. doi: 10.1016/j.jpedsurg.2015.09.022. Epub 2015 Oct 8. J Pediatr Surg. 2016. PMID: 26592955 Review.
Cited by
-
Management of intussusception in children: A systematic review.J Pediatr Surg. 2021 Mar;56(3):587-596. doi: 10.1016/j.jpedsurg.2020.09.055. Epub 2020 Oct 6. J Pediatr Surg. 2021. PMID: 33158508 Free PMC article.
-
Acute colocolic intussusception: A rare pediatric presentation.Radiol Case Rep. 2024 Nov 4;20(1):505-508. doi: 10.1016/j.radcr.2024.10.057. eCollection 2025 Jan. Radiol Case Rep. 2024. PMID: 39559498 Free PMC article.
-
Reduction of intussusception: defining a better index of successful non-operative treatment.Pediatr Radiol. 2013 Jun;43(6):649-56. doi: 10.1007/s00247-012-2552-6. Epub 2012 Dec 20. Pediatr Radiol. 2013. PMID: 23254683 Review.
-
Primary ileoileal intussusception without a lead point simulating appendicular mass in a 4-year-old girl.BMJ Case Rep. 2014 Mar 14;2014:bcr2013203390. doi: 10.1136/bcr-2013-203390. BMJ Case Rep. 2014. PMID: 24632906 Free PMC article. No abstract available.
References
-
- Daneman A, Navarro O. Intussusception. Part 1. A review of diagnostic approaches. Pediatr Radiol 2003;33:79–85 - PubMed
-
- Daneman A, Navarro O. Intussusception. Part 2. An update on the evolution of management. Pediatr Radiol 2004;34:97–108; quiz 187 - PubMed
-
- Kaiser AD, Applegate KE, Ladd AP. Current success in the treatment of intussusception in children. Surgery 2007;142:469–75; discussion 475–7 - PubMed
-
- Ko HS, Schenk JP, Troger J, Rohrschneider WK. Current radiological management of intussusception in children. Eur Radiol 2007;17:2411–21 - PubMed
-
- Barr LL, Stansberry SD, Swischuk LE. Significance of age, duration, obstruction and the dissection sign in intussusception. Pediatr Radiol 1990;20:454–6 - PubMed
