

Comparison of mammography, sonography, MRI and clinical examination in patients with locally advanced or inflammatory breast cancer who underwent neoadjuvant chemotherapy
- PMID: 21081579
- PMCID: PMC3473500
- DOI: 10.1259/bjr/74430952
Comparison of mammography, sonography, MRI and clinical examination in patients with locally advanced or inflammatory breast cancer who underwent neoadjuvant chemotherapy
Abstract
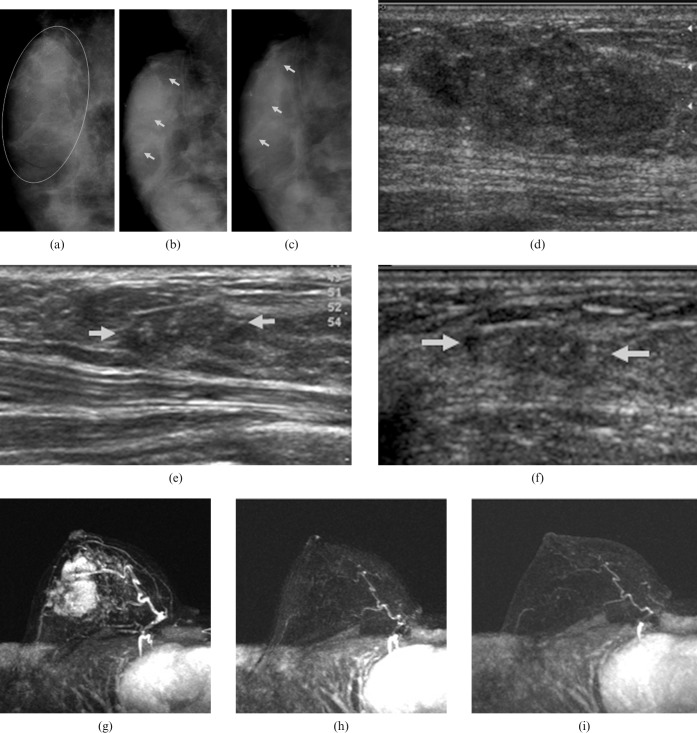
Objectives: The purpose of this study was to determine the relative accuracies of mammography, sonography, MRI and clinical examination in predicting residual tumour size and pathological response after neoadjuvant chemotherapy for locally advanced or inflammatory breast cancer. Each prediction method was compared with the gold standard of surgical pathology.
Methods: 43 patients (age range, 25-62 years; mean age, 42.7 years) with locally advanced or inflammatory breast cancer who had been treated by neoadjuvant chemotherapy were enrolled prospectively. We compared the predicted residual tumour size and the predicted response on imaging and clinical examination with residual tumour size and response on pathology. Statistical analysis was performed using weighted kappa statistics and intraclass correlation coefficients (ICC).
Results: The ICC values between predicted tumour size and pathologically determined tumour size were 0.65 for clinical examination, 0.69 for mammography, 0.78 for sonography and 0.97 for MRI. Agreement between the response predictions at mid-treatment and the responses measured by pathology had kappa values of 0.28 for clinical examination, 0.32 for mammography, 0.46 for sonography and 0.68 for MRI. Agreement between the final response predictions and the responses measured by pathology had kappa values of 0.43 for clinical examination, 0.44 for mammography, 0.50 for sonography and 0.82 for MRI.
Conclusion: Predictions of response and residual tumour size made on MRI were better correlated with the assessments of response and residual tumour size made upon pathology than were predictions made on the basis of clinical examination, mammography or sonography. Thus, the evaluation of predicted response using MRI could provide a relatively sensitive early assessment of chemotherapy efficacy.
Figures
References
-
- Bonadonna G, Valagussa P. Primary chemotherapy in operable breast cancer. Semin Oncol 1996;23:464–74 - PubMed
-
- Newman L, Buzdar A, Singletary S, Kuerer H, Buchholz T, Ames F, et al. A prospective trial of preoperative chemotherapy in resectable breast cancer: predictors of breast-conservation therapy feasibility. Ann Surg Oncol 2002;9:228–34 - PubMed
-
- Kuerer H, Singletary S, Buzdar A, Ames F, Valero V, Buchholz T, et al. Surgical conservation planning after neoadjuvant chemotherapy for stage II and operable stage III breast carcinoma. Am J Surg 2001;182:601–8 - PubMed
-
- Vlastos G, Mirza N, Lenert J, Hunt K, Ames F, Feig B, et al. The feasibility of minimally invasive surgery for stage IIA, IIB, and IIIA breast carcinoma patients after tumour downstaging with induction chemotherapy. Cancer 2000;88:1417–24 - PubMed
-
- Booser D, Hortobagyi G. Treatment of locally advanced breast cancer. Semin Oncol 1992;19:278–85 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
