

Adoption, non-adoption, and abandonment of a personal electronic health record: case study of HealthSpace
- PMID: 21081595
- PMCID: PMC2982892
- DOI: 10.1136/bmj.c5814
Adoption, non-adoption, and abandonment of a personal electronic health record: case study of HealthSpace
Abstract
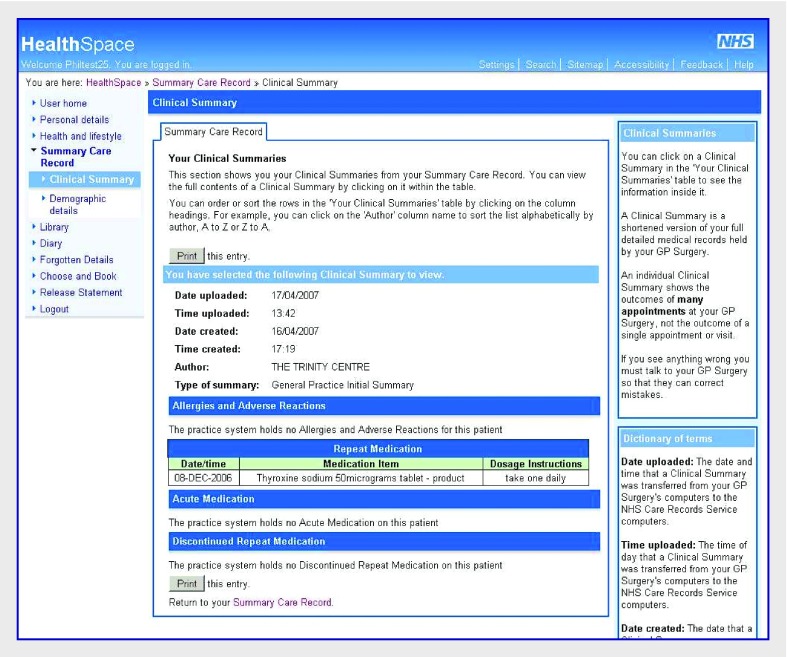
Objective: To evaluate the policy making process, implementation by NHS organisations, and patients' and carers' experiences of efforts to introduce an internet accessible personal electronic health record (HealthSpace) in a public sector healthcare system.
Design: Mixed method, multilevel case study.
Setting: English National Health Service; the basic HealthSpace technology (available throughout England) and the advanced version (available in a few localities where this option had been introduced) were considered.
Main outcome measures: National statistics on invitations sent, HealthSpace accounts created, and interviews and ethnographic observation of patients and carers. Data analysis was informed by a socio-technical approach which considered macro and micro influences on both adoption and non-adoption of innovations, and by the principles of critical discourse analysis.
Participants: 56 patients and carers (of whom 21 opened a basic HealthSpace account, 20 had diabetes but were not initially using HealthSpace, and 15 used advanced HealthSpace accounts to exchange messages with their general practitioner), 3000 pages of documents (policies, strategies, business plans, minutes of meetings, correspondence), observational field notes, and 160 interviews with policy makers, project managers, and clinical staff.
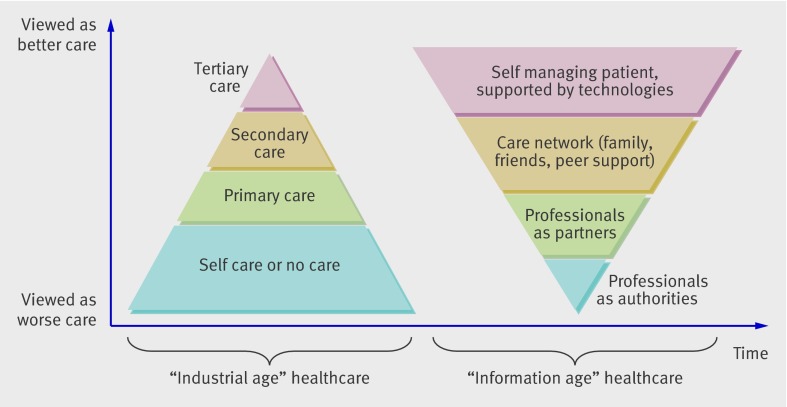
Results: Between 2007 and October 2010, 172 950 people opened a basic HealthSpace account. 2913 (0.13% of those invited) opened an advanced account, compared with 5-10% of the population anticipated in the original business case. Overall, patients perceived HealthSpace as neither useful nor easy to use and its functionality aligned poorly with their expectations and self management practices. Those who used email-style messaging were positive about its benefits, but enthusiasm beyond three early adopter clinicians was low, and fewer than 100 of 30 000 patients expressed interest. Policy makers' hopes that "deploying" HealthSpace would lead to empowered patients, personalised care, lower NHS costs, better data quality, and improved health literacy were not realised over the three year evaluation period.
Conclusion: Unless personal electronic health records align closely with people's attitudes, self management practices, identified information needs, and the wider care package (including organisational routines and incentive structures for clinicians), the risk that they will be abandoned or not adopted at all is substantial. Conceptualising such records dynamically (as components of a socio-technical network) rather than statically (as containers for data) and employing user centred design techniques might improve their chances of adoption and use. The findings raise questions about how eHealth programmes in England are developed and approved at policy level.
Conflict of interest statement
Competing interests: All authors have completed the Unified Competing Interest form at
Figures
Comment in
-
Abandoned HealthSpace. Sharing access might increase engagement.BMJ. 2010 Dec 20;341:c7209. doi: 10.1136/bmj.c7209. BMJ. 2010. PMID: 21172980 No abstract available.
-
It's a great idea and workable.BMJ. 2010 Dec 20;341:c7211. doi: 10.1136/bmj.c7211. BMJ. 2010. PMID: 21172981 No abstract available.
-
Abandoned HealthSpace. Smart phones may help.BMJ. 2010 Dec 20;341:c7216. doi: 10.1136/bmj.c7216. BMJ. 2010. PMID: 21172982 No abstract available.
-
Patient's view of HealthSpace.BMJ. 2010 Dec 20;341:c7219. doi: 10.1136/bmj.c7219. BMJ. 2010. PMID: 21172983 No abstract available.
References
-
- Bodenheimer T, Wagner EH, Grumbach K. Improving primary care for patients with chronic illness: the chronic care model. Part 1. JAMA 2002;288:1775-9. - PubMed
-
- Darzi A. NHS next stage review: our vision for primary and community care. Stationery Office, 2008.
-
- Cayton H. The flat-pack patient? Creating health together. Patient Educ Couns 2006;62:288-90. - PubMed
-
- Dimick C. The empowered patient. Preparing for a new patient interaction. J AHIMA 2010;81:26-31. - PubMed
-
- Szolovitz P, Doyle J, Long WJ, Kohane I, Paulker SG. Guardian angel: patient-centered health information systems. Massachussetts Institute of Technology, 1994.
MeSH terms
LinkOut - more resources
Full Text Sources