

Contemporary diagnostic imaging modalities for the staging and surveillance of melanoma patients: a meta-analysis
- PMID: 21081714
- PMCID: PMC3022618
- DOI: 10.1093/jnci/djq455
Contemporary diagnostic imaging modalities for the staging and surveillance of melanoma patients: a meta-analysis
Abstract
Background: Meta-analyses were performed to examine the utility of ultrasonography, computed tomography (CT), positron emission tomography (PET), and a combination of both (PET-CT) for the staging and surveillance of melanoma patients.
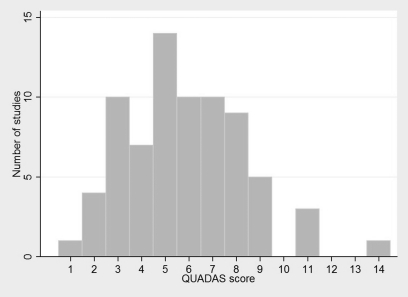
Method: Patient-level data from 74 studies containing 10,528 patients (between January 1, 1990, and June, 30, 2009) were used to derive characteristics of the diagnostic tests used. Meta-analyses were conducted by use of Bayesian bivariate binomial models to estimate sensitivity and specificity. Diagnostic odds ratios [ie, true-positive results/false-negative results)/(false-positive results/true-negative results)] and their 95% credible intervals (CrIs) and positive predictive values were used as indicators of test performance.
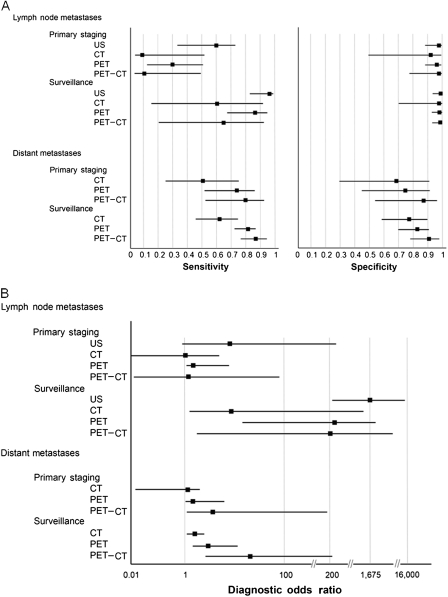
Results: Among the four imaging methods examined for the staging of regional lymph nodes, ultrasonography had the highest sensitivity (60%, 95% CrI = 33% to 83%), specificity (97%, 95% CrI = 88% to 99%), and diagnostic odds ratio (42, 95% CrI = 8.08 to 249.8). For staging of distant metastases, PET-CT had the highest sensitivity (80%, 95% CrI = 53% to 93%), specificity (87%, 95% CrI = 54% to 97%), and diagnostic odds ratio (25, 95% CrI = 3.58 to 198.7). Similar trends were observed for melanoma surveillance of lymph node involvement, with ultrasonography having the highest sensitivity (96%, 95% CrI = 85% to 99%), specificity (99%, 95% CrI = 95% to 100%), and diagnostic odds ratio (1675, 95% CrI = 226.6 to 15,920). For distant metastases, PET-CT had the highest sensitivity (86%, 95% CrI = 76% to 93%), specificity (91%, 95% CrI = 79% to 97%), and diagnostic odds ratio (67, 95% CrI = 20.42 to 229.7). Positive predictive values were likewise highest for ultrasonography in lymph node staging and for PET-CT in detecting distant metastases.
Conclusion: Among the compared modalities, ultrasonography was superior for detecting lymph node metastases, and PET-CT was superior for the detection of distant metastases in both the staging and surveillance of melanoma patients.
Figures
References
-
- American Joint Committee on Cancer. New York, NY: Springer; 2009. Melanoma of the Skin; pp. 325–344. In: Edge SB, Byrd DR, Compton CC, et al. eds. AJCC Cancer Staging Manual. 7th ed.
-
- National Comprehensive Cancer Network: Clinical Practice Guidelines in Oncology. http://www.nccn.org/professionals/physician_gls/def/ault.asp.
-
- Aloia TA, Gershenwald JE, Andtbacka RH, et al. Utility of computed tomography and magnetic resonance imaging staging before completion lymphadenectomy in patients with sentinel lymph node-positive melanoma. J Clin Oncol. 2006;24(18):2858–2865. - PubMed
-
- Balch CM, Cascinelli N. Sentinel-node biopsy in melanoma. N Engl J Med. 2006;355(13):1370–1371. - PubMed
-
- Sanki A, Uren RF, Moncrieff M, et al. Targeted high-resolution ultrasound is not an effective substitute for sentinel lymph node biopsy in patients with primary cutaneous melanoma. J Clin Oncol. 2009;27(33):5614–5619. - PubMed
