

Acupuncture in critically ill patients improves delayed gastric emptying: a randomized controlled trial
- PMID: 21081772
- PMCID: PMC3133450
- DOI: 10.1213/ANE.0b013e3181fdfac8
Acupuncture in critically ill patients improves delayed gastric emptying: a randomized controlled trial
Abstract
Background: Malnutrition remains a severe problem in the recovery of critically ill patients and leads to increased in-hospital morbidity and in-hospital stay. Even though early enteral nutrition has been shown to improve overall patient outcomes in the intensive care unit (ICU), tubefeed administration is often complicated by delayed gastric emptying and gastroesophageal reflux. Acupuncture has been successfully used in the treatment and prevention of perioperative nausea and vomiting. In this study we evaluated whether acupuncture can improve gastric emptying in comparison with standard promotility drugs in critically ill patients receiving enteral feeding.
Methods: Thirty mechanically ventilated neurosurgical ICU patients with delayed gastric emptying, defined as a gastric residual volume (GRV) >500 mL for ≥ 2 days, were prospectively and randomly assigned to either the acupoint stimulation group (ASG; bilateral transcutaneous electrical acupoint stimulation at Neiguan, PC-6) or the conventional promotility drug treatment group (DTG) over a period of 6 days (metoclopramide, cisapride, erythromycin). Patients in the ASG group did not receive any conventional promotility drugs. Successful treatment (feeding tolerance) was defined as GRV <200 mL per 24 hours.
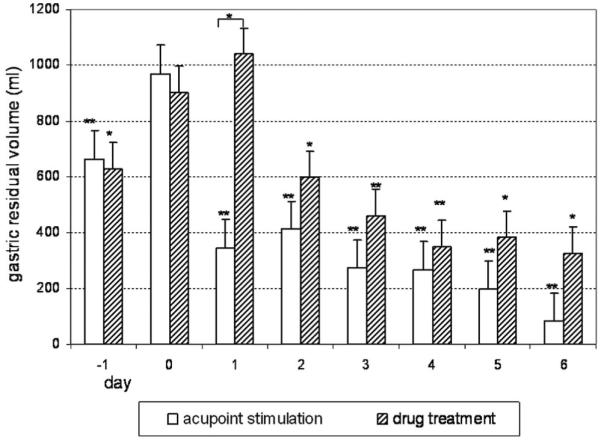
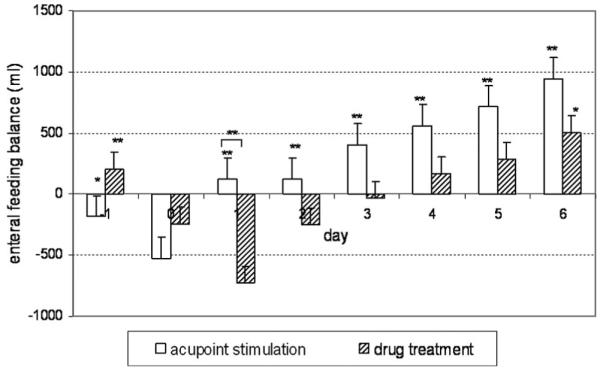
Results: Demographic and hemodynamic data were similar in both groups. After 5 days of treatment, 80% of patients in the ASG group successfully developed feeding tolerance versus 60% in the DTG group. On treatment day 1, GRV decreased from 970 ± 87 mL to 346 ± 71 mL with acupoint stimulation (P = 0.003), whereas patients in the DTG group showed a significant increase in GRV from 903 ± 60 mL to 1040 ± 211 mL (P = 0.015). In addition, GRV decreased and feeding balance (defined as enteral feeding volume minus GRV) increased in more patients in the ASG group (14 of 15) than in the DTG group (7 of 15; P = 0.014). On treatment day 1, the mean feeding balance was significantly higher in the ASG group (121 ± 128 mL) than in the DTG group (-727 ± 259 mL) (P = 0.005). Overall, the feeding balance improved significantly on all days of treatment in comparison with the DTG group. Patients in the DTG group did not show an increase in feeding balance until day 6.
Conclusions: We introduce a new protocol for acupuncture administration in the critical care setting. We demonstrated that this protocol was more effective than standard promotility medication in the treatment of delayed gastric emptying in critically ill patients. Acupoint stimulation at Neiguan (PC-6) may be a convenient and inexpensive option (with few side effects) for the prevention and treatment of malnutrition in critically ill patients.
Figures
References
-
- Peter JV, Moran JL, Phillips-Hughes J. A meta-analysis of treatment outcomes of early enteral versus early parenteral nutrition in hospitalized patients. Crit Care Med. 2005;33:213–20. - PubMed
-
- Heyland DK, Dhaliwal R. Early enteral nutrition vs. early parenteral nutrition: an irrelevant question for the critically ill? Crit Care Med. 2005;33:260–1. - PubMed
-
- Braunschweig CL, Levy P, Sheean PM, Wang X. Enteral compared with parenteral nutrition: a meta-analysis. Am J Clin Nutr. 2001;74:534–42. - PubMed
-
- Nguyen NQ, Fraser RJ, Bryant LK, Burgstad C, Chapman MJ, Bellon M, Wishart J, Holloway R, Horowitz M. The impact of delaying enteral feeding on gastric emptying, plasma cholecystokinin, and peptide YY concentrations in critically ill patients. Crit Care Med. 2008;36:1469–74. - PubMed
-
- Montejo JC, Grau T, Acosta J, Ruiz-Santana S, Planas M, Garcia-De-Lorenzo A, Mesejo A, Cervera M, Sanchez-Alvarez C, Nunez-Ruiz R, Lopez-Martinez J. Multicenter, prospective, randomized, single-blind study comparing the efficacy and gastrointestinal complications of early jejunal feeding with early gastric feeding in critically ill patients. Crit Care Med. 2002;30:796–800. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
