

Helical TomoTherapy versus sterotactic Gamma Knife radiosurgery in the treatment of single and multiple brain tumors: a dosimetric comparison
- PMID: 21081881
- PMCID: PMC5720417
- DOI: 10.1120/jacmp.v11i4.3245
Helical TomoTherapy versus sterotactic Gamma Knife radiosurgery in the treatment of single and multiple brain tumors: a dosimetric comparison
Abstract
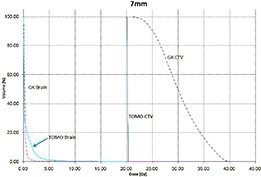
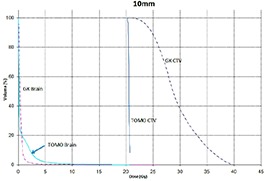
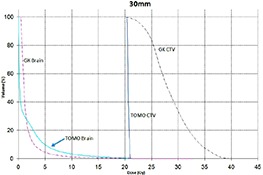
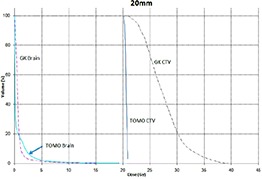
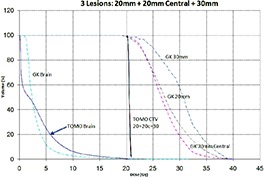
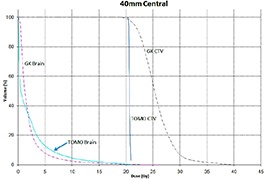
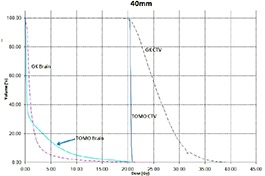
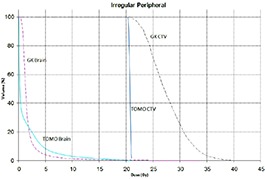
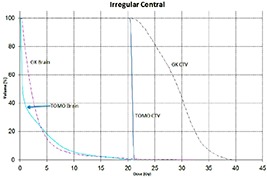
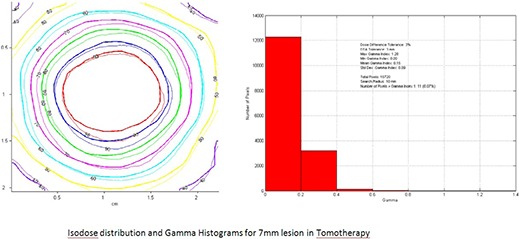
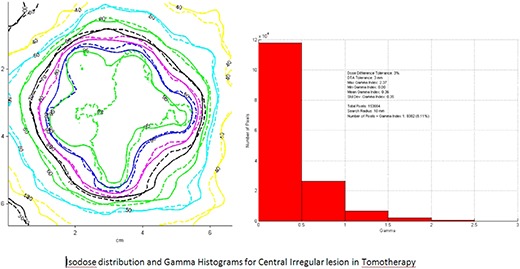
The objective was to compare the dosimetry of Helical TomoTherapy (TOMO) and Gamma Knife (GK) treatment plans for tumor and normal brain in the treatment of single and multiple brain tumors. An anthropomorphic Rando Head phantom was used to compare the dosimetry of TOMO and GK. Eight brain tumors of various shapes, sizes and locations were used to generate 10 plans. The radiation dose was 20 Gy prescribed to the 100% isodose line for TOMO plans and to the 50% for the GK plans. Dose Volume Histograms for tumor and brain were compared. Equivalent Uniform Dose (gEUD), Tumor Control Probability (TCP) and Normal Tissue Complication Probability (NTCP) were performed and used for plan comparisons. Average minimum, mean, median and maximum tumor doses were 19.93, 27.83, 27.38, 39.60 Gy for GK and 20.17, 20.60, 20.59, 20.90 Gy for TOMO. Average gEUD values for tumor and normal brain were 25.0 and 7.2 Gy for GK and 20.7 and 8.1 Gy for TOMO. Conformity indices (CI) were similar for both modalities. Gradient indices (GI) were greater for TOMO. A combination plan was also generated using all eight tumors. TOMO was able to target all eight tumors simultaneously resulting in mean tumor and brain doses of 20.5 and 9.35 Gy, respectively. Due to the maximum limit of 50 beams per plan, GK was unable to provide a treatment plan for all eight tumors. GK provides an advantage for all tumor sizes with respect to tumor and normal brain dose. Clinical studies are needed to correlate these dosimetric findings with patient outcomes.
Figures
References
-
- Aragon‐Ching JB, Zujewski JA. CNS metastasis: an old problem in a new guise. Clin Cancer Res. 2007;13(6):1644–47. - PubMed
-
- Andrews DW, Scott CB, Sperduto PW, et al. Whole brain radiation therapy with or without stereotactic radiosurgery boost for patients with one to three brain metastases: phase III results of the RTOG 9508 randomized trial. Lancet. 2004;363(9422):1665–72. - PubMed
-
- Aoyama H, Shirato H, Tago M, et al. Stereotactic radiosurgery plus whole‐brain radiation therapy vs stereotactic radiosurgery alone for treatment of brain metastases: a randomized controlled trial. JAMA. 2006;295(21):2483–91. - PubMed
-
- Bhatnagar AK, Flickinger JC, Kondziolka D, Lunsford LD. Stereotactic radiosurgery for four or more intracranial metastases. Int J Radiat Oncol Biol Phys. 2006;64(3):898–903. - PubMed
-
- Rades D, Kueter JD, Pluemer A, Veninga T, Schild SE. Matched‐pair analysis comparing whole‐brain radiotherapy plus stereotactic radiosurgery versus surgery plus whole‐brain radiotherapy and a boost to the metastatic site for one or two brain metastases. Int J Radiat Oncol Biol Phys. 2009;73(4):1077–81. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
