

Analysis of complications following decompressive craniectomy for traumatic brain injury
- PMID: 21082053
- PMCID: PMC2966727
- DOI: 10.3340/jkns.2010.48.3.244
Analysis of complications following decompressive craniectomy for traumatic brain injury
Abstract
Objective: Adequate management of increased intracranial pressure (ICP) is critical in patients with traumatic brain injury (TBI), and decompressive craniectomy is widely used to treat refractory increased ICP. The authors reviewed and analyzed complications following decompressive craniectomy for the management of TBI.
Methods: A total of 89 consecutive patients who underwent decompressive craniectomy for TBI between February 2004 and February 2009 were reviewed retrospectively. Incidence rates of complications secondary to decompressive craniectomy were determined, and analyses were performed to identify clinical factors associated with the development of complications and the poor outcome.
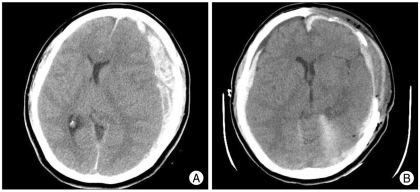
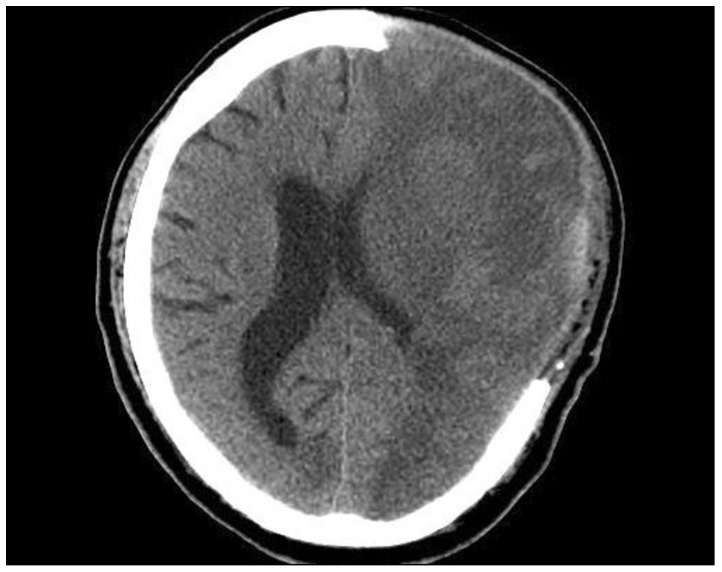
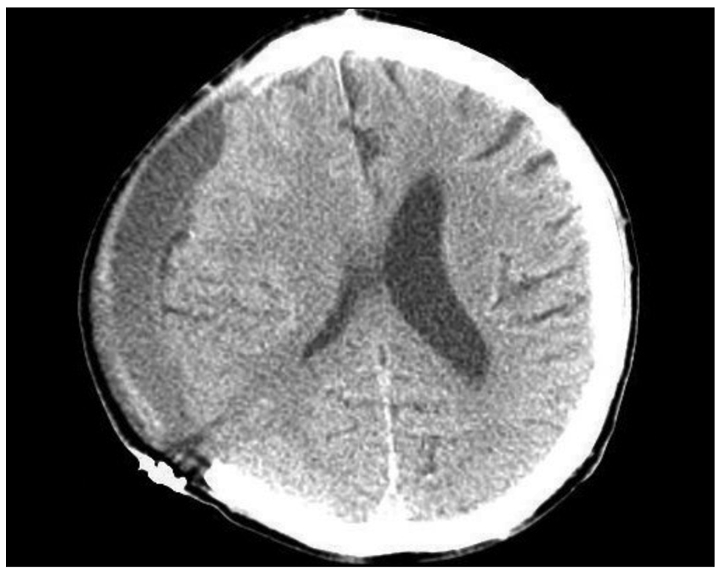
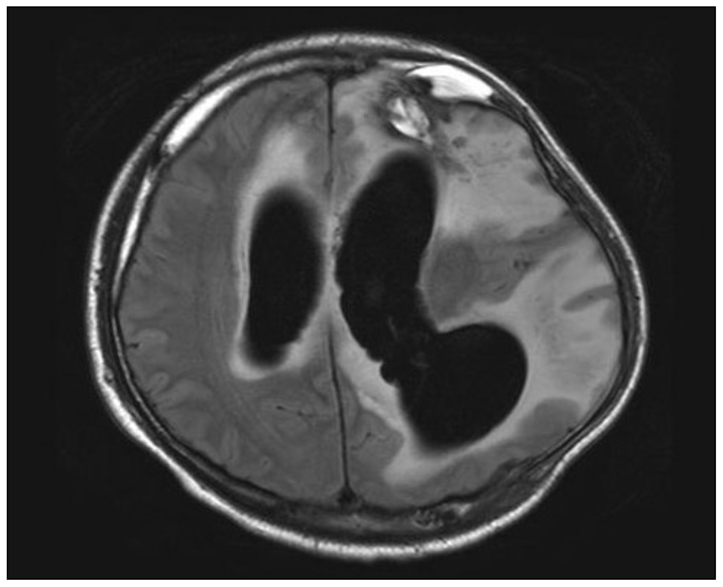
Results: Complications secondary to decompressive craniectomy occurred in 48 of the 89 (53.9%) patients. Furthermore, these complications occurred in a sequential fashion at specific times after surgical intervention; cerebral contusion expansion (2.2 ± 1.2 days), newly appearing subdural or epidural hematoma contralateral to the craniectomy defect (1.5 ± 0.9 days), epilepsy (2.7 ± 1.5 days), cerebrospinal fluid leakage through the scalp incision (7.0 ± 4.2 days), and external cerebral herniation (5.5 ± 3.3 days). Subdural effusion (10.8 ± 5.2 days) and postoperative infection (9.8 ± 3.1 days) developed between one and four weeks postoperatively. Trephined and post-traumatic hydrocephalus syndromes developed after one month postoperatively (at 79.5 ± 23.6 and 49.2 ± 14.1 days, respectively).
Conclusion: A poor GCS score (≤ 8) and an age of ≥ 65 were found to be related to the occurrence of one of the above-mentioned complications. These results should help neurosurgeons anticipate these complications, to adopt management strategies that reduce the risks of complications, and to improve clinical outcomes.
Keywords: Complication; Decompressive craniectomy; Traumatic brain injury.
Figures
References
-
- Aarabi B, Hesdorffer DC, Ahn ES, Aresco C, Scalea TM, Eisenberg HM. Outcome following decompressive craniectomy for malignant swelling due to severe head injury. J Neurosurg. 2006;104:469–479. - PubMed
-
- Albanèse J, Leone M, Alliez JR, Kaya JM, Antonini F, Alliez B, et al. Decompressive craniectomy for severe traumatic brain injury : Evaluation of the effects at one year. Crit Care Med. 2003;31:2535–2538. - PubMed
-
- Boret H, Fesselet J, Meaudre E, Gaillard PE, Cantais E. Cerebral microdialysis and P(ti)O2 for neuro-monitoring before decompressive craniectomy. Acta Anaesthesiol Scand. 2006;50:252–254. - PubMed
-
- Carvi Y Nievas MN, Hollerhage HG. Early combined cranioplasty and programmable shunt in patients with skull bone defects and CSF-circulation disorders. Neurol Res. 2006;28:139–144. - PubMed
-
- Chen JW, Ruff RL, Eavery R, Wasterlain CG. Posttraumatic epilepsy and treatment. J Rehabil Res Dev. 2009;46:685–696. - PubMed
LinkOut - more resources
Full Text Sources
