

Disturbance of glucose homeostasis after pediatric cardiac surgery
- PMID: 21082177
- PMCID: PMC3033526
- DOI: 10.1007/s00246-010-9829-z
Disturbance of glucose homeostasis after pediatric cardiac surgery
Abstract
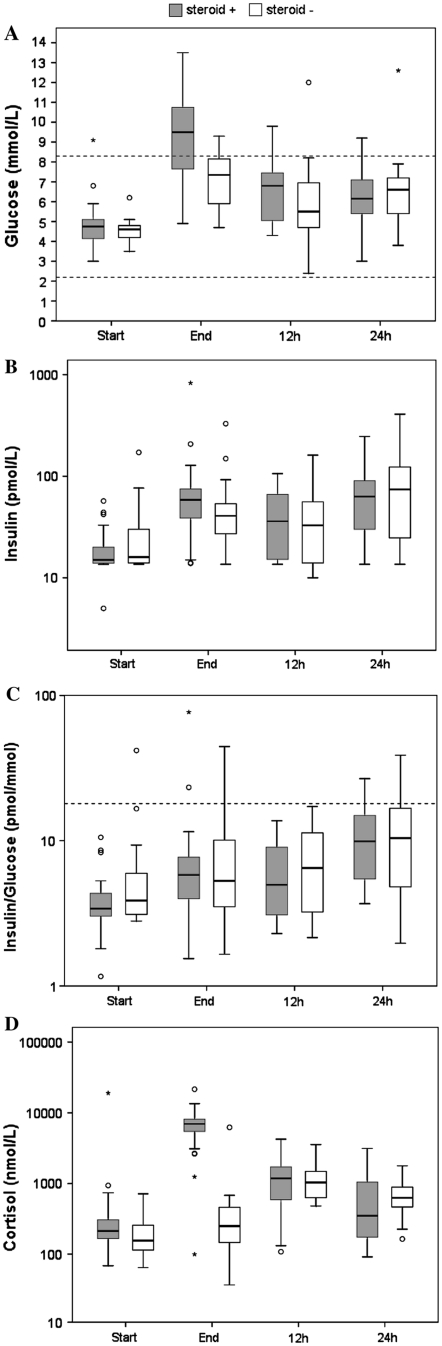
This study aimed to evaluate the time course of perioperative blood glucose levels of children undergoing cardiac surgery for congenital heart disease in relation to endogenous stress hormones, inflammatory mediators, and exogenous factors such as caloric intake and glucocorticoid use. The study prospectively included 49 children undergoing cardiac surgery. Blood glucose levels, hormonal alterations, and inflammatory responses were investigated before and at the end of surgery, then 12 and 24 h afterward. In general, blood glucose levels were highest at the end of surgery. Hyperglycemia, defined as a glucose level higher than 8.3 mmol/l (>150 mg/dl) was present in 52% of the children at the end of surgery. Spontaneous normalization of blood glucose occurred in 94% of the children within 24 h. During surgery, glucocorticoids were administered to 65% of the children, and this was the main factor associated with hyperglycemia at the end of surgery (determined by univariate analysis of variance). Hyperglycemia disappeared spontaneously without insulin therapy after 12-24 h for the majority of the children. Postoperative morbidity was low in the study group, so the presumed positive effects of glucocorticoids seemed to outweigh the adverse effects of iatrogenic hyperglycemia.
Figures
References
-
- Bouwmeester NJ, Anand KJ, van Dijk M, Hop WC, Boomsma F, Tibboel D. Hormonal and metabolic stress responses after major surgery in children aged 0–3 years: a double-blind, randomized trial comparing the effects of continuous versus intermittent morphine. Br J Anaesth. 2001;87:390–399. doi: 10.1093/bja/87.3.390. - DOI - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
