

T cell infiltrate and outcome following resection of intermediate-grade primary neuroendocrine tumours and liver metastases
- PMID: 21083792
- PMCID: PMC3003477
- DOI: 10.1111/j.1477-2574.2010.00231.x
T cell infiltrate and outcome following resection of intermediate-grade primary neuroendocrine tumours and liver metastases
Abstract
Background: Tumour-infiltrating lymphocytes (TILs) have been shown to predict survival in numerous malignancies. The importance of TILs in primary pancreatic neuroendocrine tumours (NETs) and NET liver metastases (NETLMs) has not been defined.
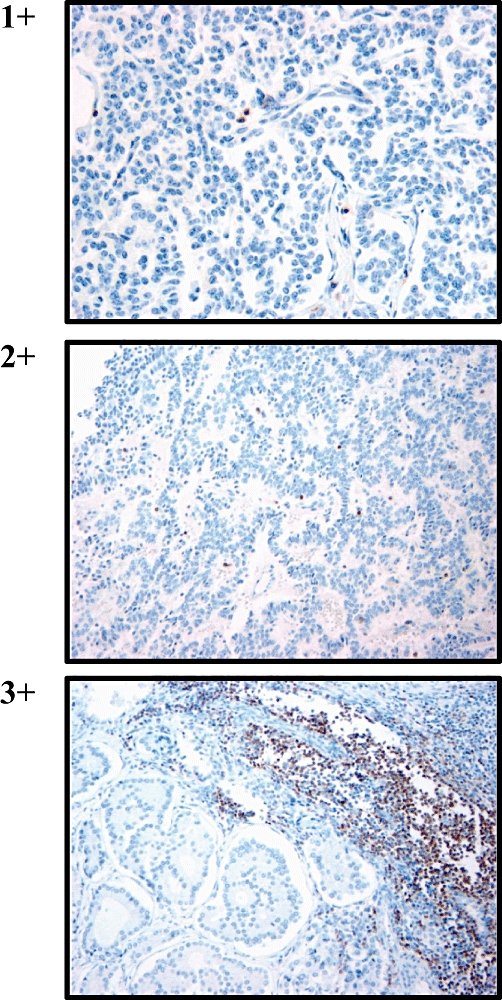
Methods: We identified 87 patients with NETs and 39 with NETLMs who had undergone resection. Immunohistochemistry was performed to determine TIL counts. Recurrence-free survival (RFS) and overall survival (OS) were determined using the log-rank test.
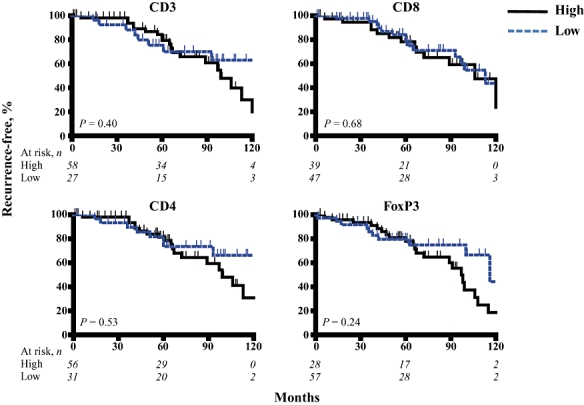
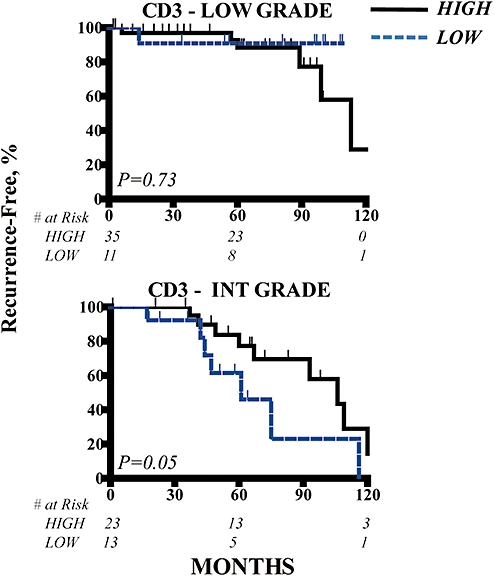
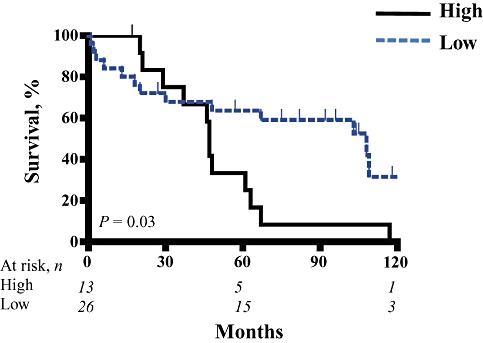
Results: The median follow-up time was 62 months in NET patients and 48 months in NETLM patients. Vascular invasion and histologic grade were the only independent predictors of outcome for NETs and NETLMs, respectively. Analysis of intermediate-grade NETs indicated that a dense T cell (CD3+) infiltrate was associated with a median RFS of 128 months compared with 61 months for those with low levels of intratumoral T cells (P= 0.05, univariate analysis). Examination of NETLMs revealed that a low level of infiltrating regulatory T cells (Treg, FoxP3+) was a predictor of prolonged survival (P < 0.01, univariate analysis).
Conclusions: A robust T cell infiltrate is associated with improved RFS following resection of intermediate-grade NETs, whereas the presence of more Treg correlated with shorter OS after treatment of NETLMs. Further study of the immune response to intermediate-grade NETs and NETLMs is warranted.
Figures
References
-
- Fahy BN, D'Angelica M, DeMatteo RP, Blumgart LH, Weiser MR, Ostrovnaya I, et al. Synchronous hepatic metastases from colon cancer: changing treatment strategies and results of surgical intervention. Ann Surg Oncol. 2009;16:361–370. - PubMed
-
- Kulke M. Advances in the treatment of neuroendocrine tumours. Curr Treat Options Oncol. 2005;6:397–409. - PubMed
-
- Modlin IM, Sandor A. An analysis of 8305 cases of carcinoid tumours. Cancer. 1997;79:813–829. - PubMed
-
- Oberg K, Eriksson B. Medical treatment of neuroendocrine gut and pancreatic tumours. Acta Oncol. 1989;28:425–431. - PubMed
-
- Chamberlain RS, Canes D, Brown KT, Saltz L, Jarnagin W, Fong Y, Blumgart LH. Hepatic neuroendocrine metastases: does intervention alter outcomes? J Am Coll Surg. 2000;190:432–445. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
