

Antibodies to myelin oligodendrocyte glycoprotein in HIV-1 associated neurocognitive disorder: a cross-sectional cohort study
- PMID: 21083890
- PMCID: PMC2998475
- DOI: 10.1186/1742-2094-7-79
Antibodies to myelin oligodendrocyte glycoprotein in HIV-1 associated neurocognitive disorder: a cross-sectional cohort study
Abstract
Background: Neuroinflammation and demyelination have been suggested as mechanisms causing HIV-1 associated neurocognitive disorder (HAND). This cross-sectional cohort study explores the potential role of antibodies to myelin oligodendrocyte glycoprotein (MOG), a putative autoantigen in multiple sclerosis, in the pathogenesis of HAND.
Methods: IgG antibodies against MOG were measured by ELISA in sera and cerebrospinal fluid (CSF) of 65 HIV-positive patients with HAND (n = 14), cerebral opportunistic infections (HIVOI, n = 25), primary HIV infection (HIVM, n = 5) and asymptomatic patients (HIVasy, n = 21). As control group HIV-negative patients with bacterial or viral CNS infections (OIND, n = 18) and other neurological diseases (OND, n = 22) were included. In a subset of HAND patients MOG antibodies were determined before and during antiviral therapy.
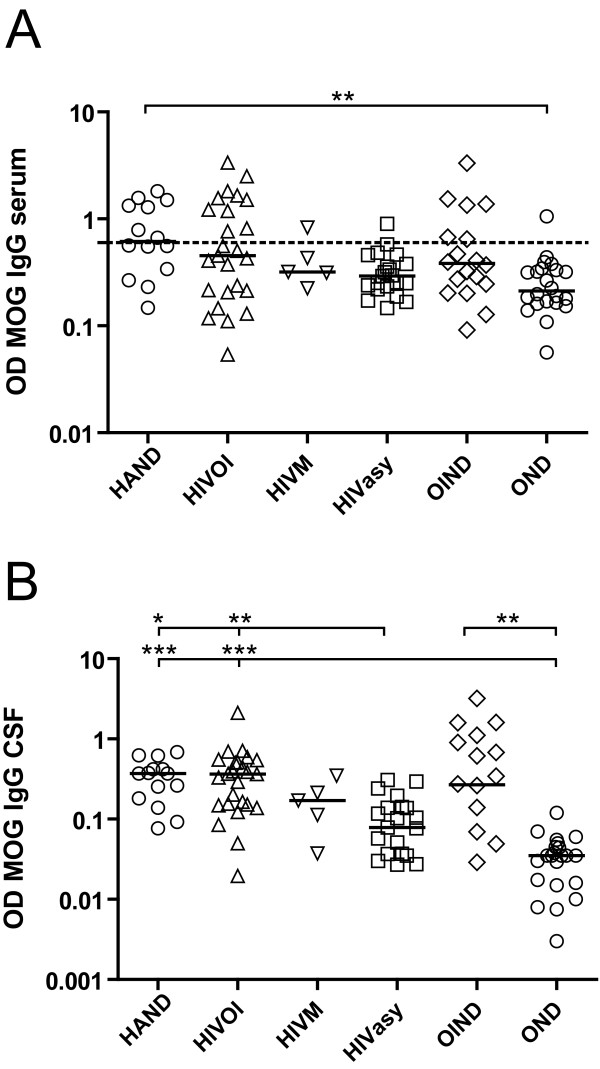
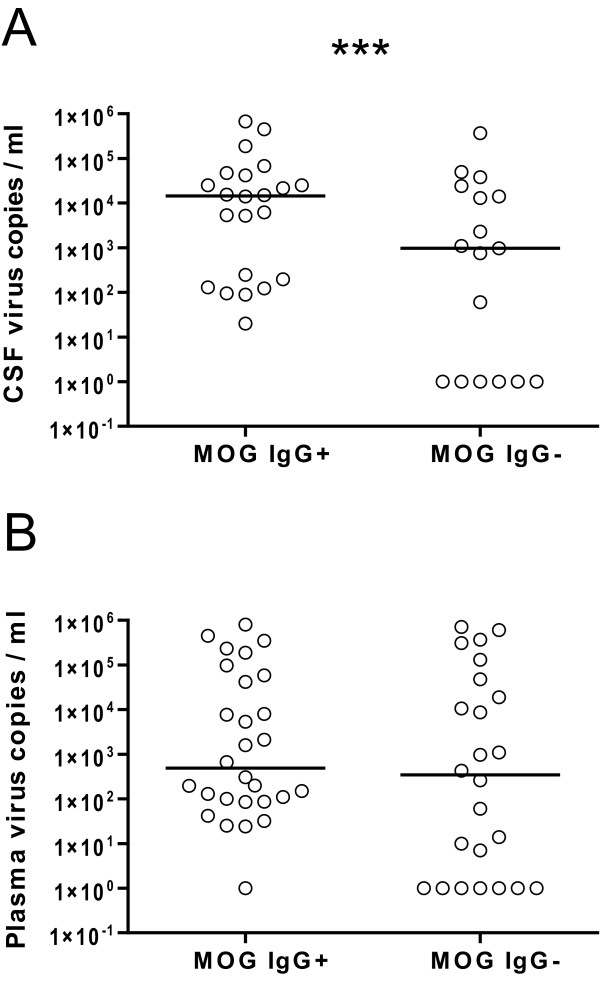
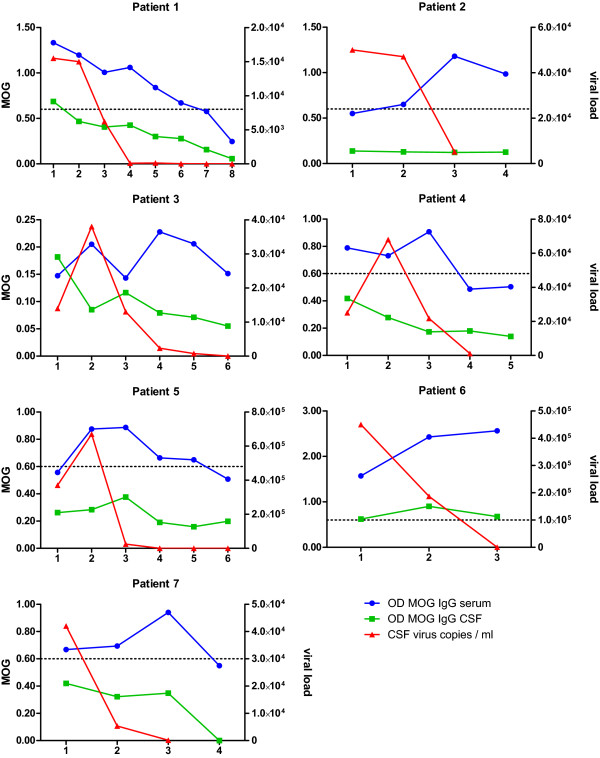
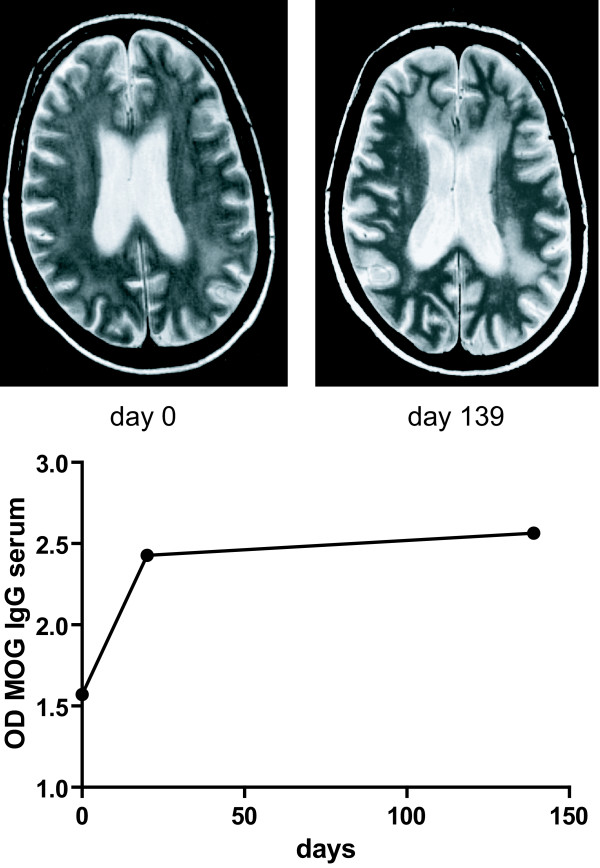
Results: In serum, significantly higher MOG antibody titers were observed in HAND compared to OND patients. In CSF, significantly higher antibody titers were observed in HAND and HIVOI patients compared to HIVasy and OND patients and in OIND compared to OND patients. CSF anti-MOG antibodies showed a high sensitivity and specificity (85.7% and 76.2%) for discriminating patients with active HAND from asymptomatic HIV patients. MOG immunopositive HAND patients performed significantly worse on the HIV dementia scale and showed higher viral load in CSF. In longitudinally studied HAND patients, sustained antibody response was noted despite successful clearance of viral RNA.
Conclusions: Persistence of MOG antibodies despite viral clearance in a high percentage of HAND patients suggests ongoing neuroinflammation, possibly preventing recovery from HAND.
Figures
Similar articles
-
Antibodies against the myelin oligodendrocyte glycoprotein and the myelin basic protein in multiple sclerosis and other neurological diseases: a comparative study.Brain. 1999 Nov;122 ( Pt 11):2047-56. doi: 10.1093/brain/122.11.2047. Brain. 1999. PMID: 10545390 Clinical Trial.
-
Anti-MOG autoantibodies in Italian multiple sclerosis patients: specificity, sensitivity and clinical association.Int Immunol. 2004 Apr;16(4):559-65. doi: 10.1093/intimm/dxh056. Int Immunol. 2004. PMID: 15039386
-
Identification of a pathogenic antibody response to native myelin oligodendrocyte glycoprotein in multiple sclerosis.Proc Natl Acad Sci U S A. 2006 Dec 12;103(50):19057-62. doi: 10.1073/pnas.0607242103. Epub 2006 Dec 1. Proc Natl Acad Sci U S A. 2006. PMID: 17142321 Free PMC article.
-
Myelin oligodendrocyte glycoprotein: a novel candidate autoantigen in multiple sclerosis.J Mol Med (Berl). 1997 Feb;75(2):77-88. doi: 10.1007/s001090050092. J Mol Med (Berl). 1997. PMID: 9083925 Review.
-
The myelin oligodendrocyte glycoprotein (MOG): a model for antibody-mediated demyelination in experimental autoimmune encephalomyelitis and multiple sclerosis.J Neural Transm Suppl. 2000;(58):123-33. doi: 10.1007/978-3-7091-6284-2_10. J Neural Transm Suppl. 2000. PMID: 11128602 Review.
Cited by
-
Untreated Patients Dying With AIDS Have Loss of Neocortical Neurons and Glia Cells.Front Neurosci. 2020 Jan 15;13:1398. doi: 10.3389/fnins.2019.01398. eCollection 2019. Front Neurosci. 2020. PMID: 32009881 Free PMC article.
-
Bromodomains in Human-Immunodeficiency Virus-Associated Neurocognitive Disorders: A Model of Ferroptosis-Induced Neurodegeneration.Front Neurosci. 2022 May 12;16:904816. doi: 10.3389/fnins.2022.904816. eCollection 2022. Front Neurosci. 2022. PMID: 35645713 Free PMC article. Review.
-
Common transcriptional signatures in brain tissue from patients with HIV-associated neurocognitive disorders, Alzheimer's disease, and Multiple Sclerosis.J Neuroimmune Pharmacol. 2012 Dec;7(4):914-26. doi: 10.1007/s11481-012-9409-5. Epub 2012 Oct 12. J Neuroimmune Pharmacol. 2012. PMID: 23065460 Free PMC article. Review.
-
[HIV 1-associated neurocognitive disorder: current epidemiology, pathogenesis, diagnosis and management].Nervenarzt. 2014 Oct;85(10):1280-90. doi: 10.1007/s00115-014-4082-y. Nervenarzt. 2014. PMID: 25292163 Review. German.
-
IgG intrathecal synthesis in HIV-associated neurocognitive disorder (HAND) according to the HIV-1 subtypes and pattern of HIV RNA in CNS and plasma compartments.J Neuroimmunol. 2021 Jun 15;355:577542. doi: 10.1016/j.jneuroim.2021.577542. Epub 2021 Mar 8. J Neuroimmunol. 2021. PMID: 33845284 Free PMC article.
References
-
- Cysique LA, Maruff P, Brew BJ. Prevalence and pattern of neuropsychological impairment in human immunodeficiency virus-infected/acquired immunodeficiency syndrome (HIV/AIDS) patients across pre-and post-highly active antiretroviral therapy eras: a combined study of two cohorts. J Neurovirol. 2004;10:350–357. doi: 10.1080/13550280490521078. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Research Materials
