

Rectal laterally spreading tumors successfully treated in two steps by endoscopic submucosal dissection and endoscopic mucosal resection
- PMID: 21083919
- PMCID: PMC2994792
- DOI: 10.1186/1471-230X-10-135
Rectal laterally spreading tumors successfully treated in two steps by endoscopic submucosal dissection and endoscopic mucosal resection
Abstract
Background: Endoscopic submucosal dissection (ESD) is an advanced technique of therapeutic endoscopy alternative to endoscopic mucosal resection (EMR) for superficial gastrointestinal neoplasms >2 cm. ESD allows for the direct dissection of the submucosa and large lesions can be resected en bloc. ESD is not limited by resection size, increases histologically complete resection rates and may reduce the local recurrence. Nevertheless, the technique is time-consuming, technically demanding and associated with a high complication rate. To reduce the risk of complications, different devices and technical advances have been proposed with conflicting results and, still, ESD en bloc resections of huge lesions are associated with increased complications.
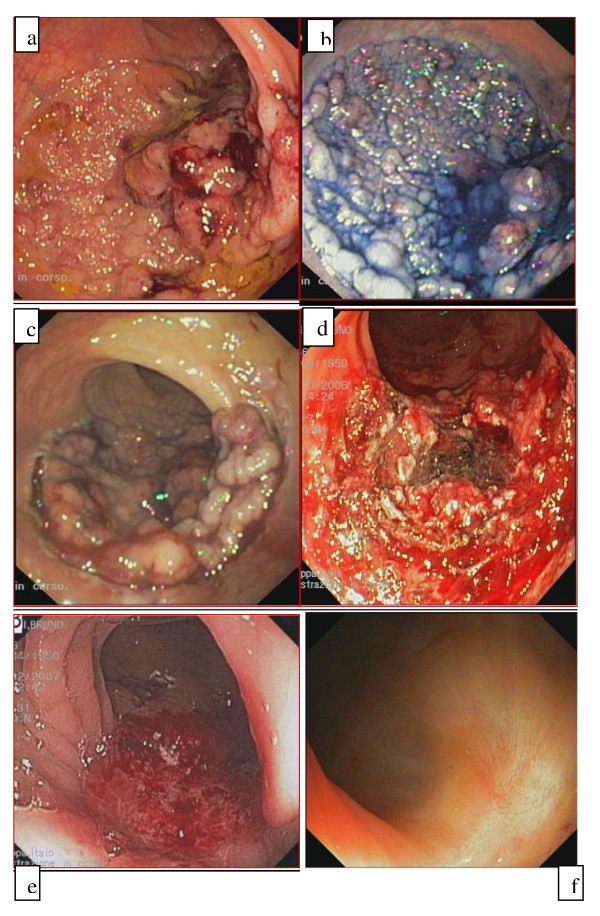
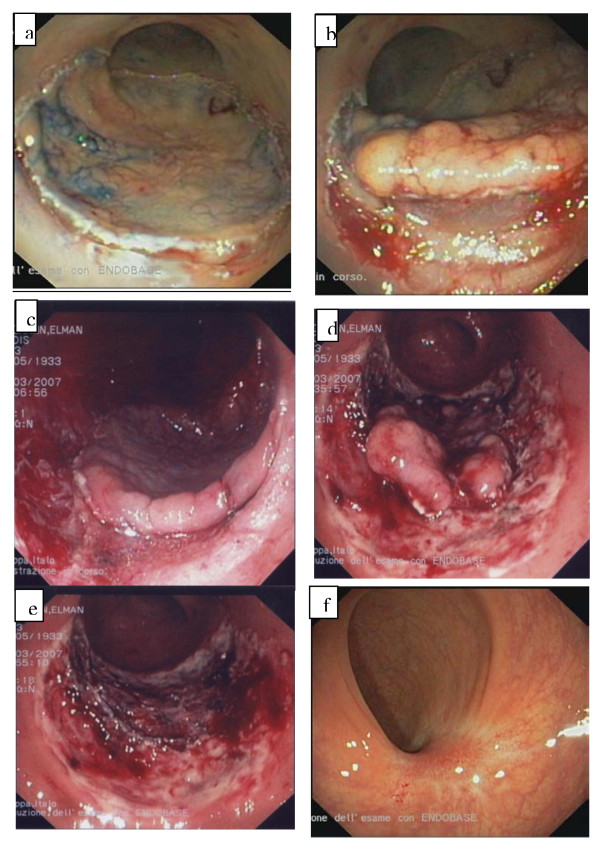
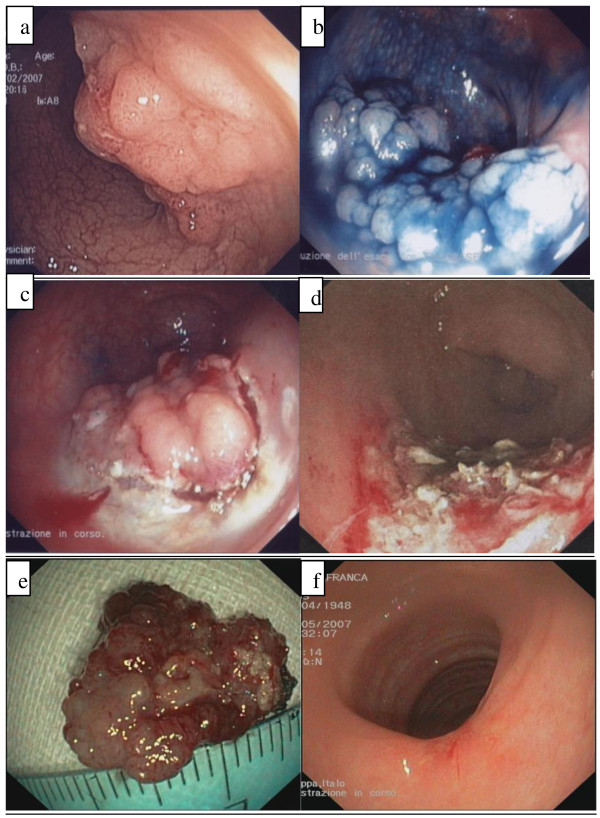
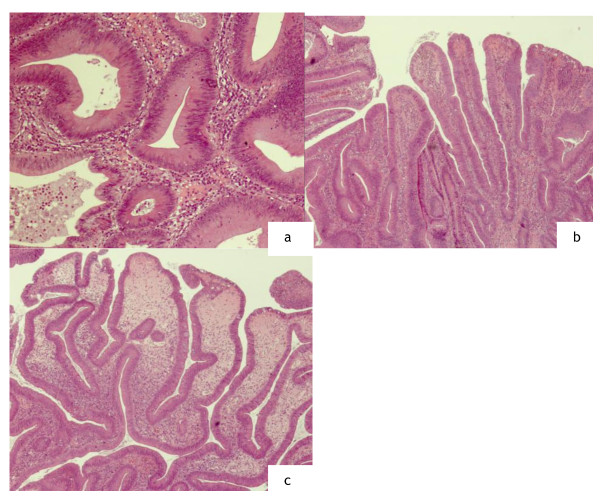
Case presentation: We successfully used a combined ESD/EMR technique for huge rectal laterally spreading tumors (LSTs). ESD was used for circumferential resection of 2/3 of the lesion followed by piecemeal resection (2-3 pieces) of the central part of the tumour. In all three patients we obtained the complete dissection of the polyp and the complete histological evaluation in absence of complications and recurrence at 6 months' follow up.
Conclusions: In the treatment of rectal LSTs, the combined treatment - ESD/EMR resection may be considered a suitable therapeutic option, indicated in selected cases as an alternative to surgery, in which the two techniques are neither reliable nor safe separately. However, to confirm our results, larger trials with longer follow up are required together with improvement of the technique and of the technical devices.
Figures
Similar articles
-
Colorectal endoscopic submucosal dissection: Technical advantages compared to endoscopic mucosal resection and minimally invasive surgery.Dig Endosc. 2014 Jan;26 Suppl 1:52-61. doi: 10.1111/den.12196. Epub 2013 Nov 5. Dig Endosc. 2014. PMID: 24191896 Review.
-
Endoscopic submucosal dissection for treatment of rectal carcinoid tumors.Gastrointest Endosc. 2010 Jul;72(1):143-9. doi: 10.1016/j.gie.2010.01.040. Epub 2010 Apr 9. Gastrointest Endosc. 2010. PMID: 20381798
-
Endoscopic submucosal dissection versus endoscopic mucosal resection for the treatment of rectal lesions involving the dentate line.Surg Endosc. 2024 Aug;38(8):4485-4495. doi: 10.1007/s00464-024-10994-6. Epub 2024 Jun 24. Surg Endosc. 2024. PMID: 38914887 Free PMC article.
-
Circumferential submucosal incision prior to endoscopic mucosal resection provides comparable clinical outcomes to submucosal dissection for well-differentiated neuroendocrine tumors of the rectum.Surg Endosc. 2015 Jun;29(6):1500-5. doi: 10.1007/s00464-014-3831-0. Epub 2014 Oct 3. Surg Endosc. 2015. PMID: 25277474
-
Endoscopic submucosal dissection (ESD) versus simplified/hybrid ESD.Gastrointest Endosc Clin N Am. 2014 Apr;24(2):191-9. doi: 10.1016/j.giec.2013.11.004. Epub 2014 Jan 25. Gastrointest Endosc Clin N Am. 2014. PMID: 24679231 Review.
Cited by
-
Experience with a new device for pathological assessment of colonic endoscopic submucosal dissection.Tech Coloproctol. 2014 Nov;18(11):1117-23. doi: 10.1007/s10151-014-1213-1. Epub 2014 Sep 12. Tech Coloproctol. 2014. PMID: 25214205
-
Ligation-assisted endoscopic enucleation for the diagnosis and resection of small gastrointestinal tumors originating from the muscularis propria: a preliminary study.BMC Gastroenterol. 2013 May 16;13:88. doi: 10.1186/1471-230X-13-88. BMC Gastroenterol. 2013. PMID: 23679863 Free PMC article.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
