

Symptomatic progression of asymptomatic rotator cuff tears: a prospective study of clinical and sonographic variables
- PMID: 21084574
- PMCID: PMC2970889
- DOI: 10.2106/JBJS.I.00506
Symptomatic progression of asymptomatic rotator cuff tears: a prospective study of clinical and sonographic variables
Abstract
Background: The purposes of this study were to identify changes in tear dimensions, shoulder function, and glenohumeral kinematics when an asymptomatic rotator cuff tear becomes painful and to identify characteristics of individuals who develop pain compared with those who remain asymptomatic.
Methods: A cohort of 195 subjects with an asymptomatic rotator cuff tear was prospectively monitored for pain development and examined annually for changes in various parameters such as tear size, fatty degeneration of the rotator cuff muscle, glenohumeral kinematics, and shoulder function. Forty-four subjects were found to have developed new pain, and the parameters before and after pain development were compared. The forty-four subjects were then compared with a group of fifty-five subjects who remained asymptomatic over a two-year period.
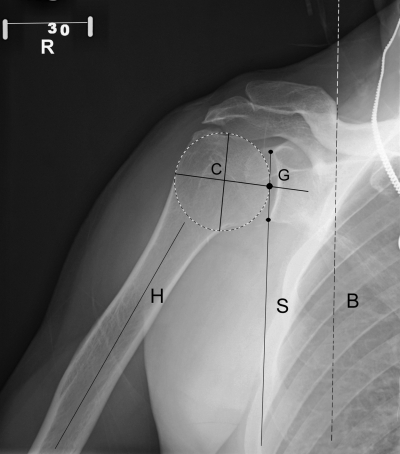
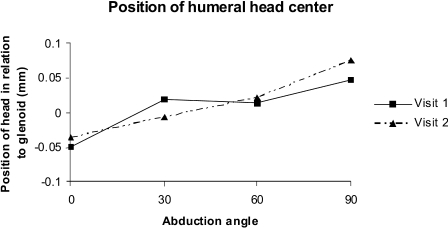
Results: With pain development, the size of a full-thickness rotator cuff tear increased significantly, with 18% of the full-thickness tears showing an increase of >5 mm, and 40% of the partial-thickness tears had progressed to a full-thickness tear. In comparison with the assessments made before the onset of pain, the American Shoulder and Elbow Surgeons scores for shoulder function were significantly decreased and all measures of shoulder range of motion were decreased except for external rotation at 90° of abduction. There was an increase in compensatory scapulothoracic motion in relation to the glenohumeral motion during early shoulder abduction with pain development. No significant changes were found in external rotation strength or muscular fatty degeneration. Compared with the subjects who remained asymptomatic, the subjects who developed pain were found to have significantly larger tears at the time of initial enrollment.
Conclusions: Pain development in shoulders with an asymptomatic rotator cuff tear is associated with an increase in tear size. Larger tears are more likely to develop pain in the short term than are smaller tears. Further research is warranted to investigate the role of prophylactic treatment of asymptomatic shoulders to avoid the development of pain and loss of shoulder function.
Figures
Comment in
-
Commentary on an article by Nathan A. Mall, MD, et al.: "Symptomatic progression of asymptomatic rotator cuff tears: a prospective study of clinical and sonographic variables".J Bone Joint Surg Am. 2010 Nov 17;92(16):e28. doi: 10.2106/JBJS.J.01200. J Bone Joint Surg Am. 2010. PMID: 21084572 No abstract available.
References
-
- Milgrom C, Schaffler M, Gilbert S, van Holsbeeck M. Rotator-cuff changes in asymptomatic adults. The effect of age, hand dominance and gender. J Bone Joint Surg Br. 1995;77:296-8 - PubMed
-
- Sher JS, Uribe JW, Posada A, Murphy BJ, Zlatkin MB. Abnormal findings on magnetic resonance images of asymptomatic shoulders. J Bone Joint Surg Am. 1995;77:10-5 - PubMed
-
- Yamaguchi K, Tetro AM, Blam O, Evanoff BA, Teefey SA, Middleton WD. Natural history of asymptomatic rotator cuff tears: a longitudinal analysis of asymptomatic tears detected sonographically. J Shoulder Elbow Surg. 2001;10:199-203 - PubMed
-
- Teefey SA, Hasan SA, Middleton WD, Patel M, Wright RW, Yamaguchi K. Ultrasonography of the rotator cuff. A comparison of ultrasonographic and arthroscopic findings in one hundred consecutive cases. J Bone Joint Surg Am. 2000;82:498-504 - PubMed
-
- Teefey SA, Rubin DA, Middleton WD, Hildebolt CF, Leibold RA, Yamaguchi K. Detection and quantification of rotator cuff tears. Comparison of ultrasonographic, magnetic resonance imaging, and arthroscopic findings in seventy-one consecutive cases. J Bone Joint Surg Am. 2004;86:708-16 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
