

Modelflow underestimates cardiac output in heat-stressed individuals
- PMID: 21084673
- PMCID: PMC3043797
- DOI: 10.1152/ajpregu.00505.2010
Modelflow underestimates cardiac output in heat-stressed individuals
Abstract
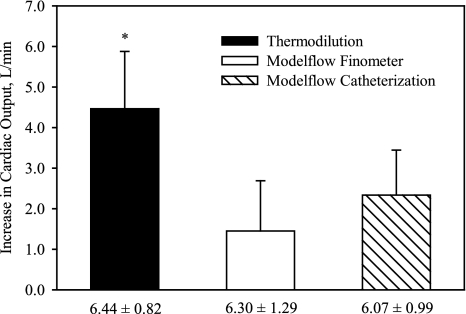
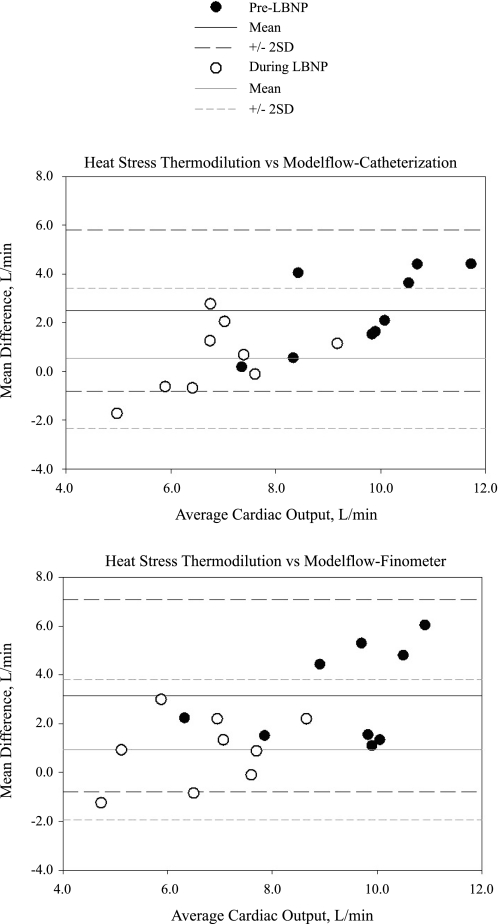
An estimation of cardiac output can be obtained from arterial pressure waveforms using the Modelflow method. However, whether the assumptions associated with Modelflow calculations are accurate during whole body heating is unknown. This project tested the hypothesis that cardiac output obtained via Modelflow accurately tracks thermodilution-derived cardiac outputs during whole body heat stress. Acute changes of cardiac output were accomplished via lower-body negative pressure (LBNP) during normothermic and heat-stressed conditions. In nine healthy normotensive subjects, arterial pressure was measured via brachial artery cannulation and the volume-clamp method of the Finometer. Cardiac output was estimated from both pressure waveforms using the Modeflow method. In normothermic conditions, cardiac outputs estimated via Modelflow (arterial cannulation: 6.1 ± 1.0 l/min; Finometer 6.3 ± 1.3 l/min) were similar with cardiac outputs measured by thermodilution (6.4 ± 0.8 l/min). The subsequent reduction in cardiac output during LBNP was also similar among these methods. Whole body heat stress elevated internal temperature from 36.6 ± 0.3 to 37.8 ± 0.4°C and increased cardiac output from 6.4 ± 0.8 to 10.9 ± 2.0 l/min when evaluated with thermodilution (P < 0.001). However, the increase in cardiac output estimated from the Modelflow method for both arterial cannulation (2.3 ± 1.1 l/min) and Finometer (1.5 ± 1.2 l/min) was attenuated compared with thermodilution (4.5 ± 1.4 l/min, both P < 0.01). Finally, the reduction in cardiac output during LBNP while heat stressed was significantly attenuated for both Modelflow methods (cannulation: -1.8 ± 1.2 l/min, Finometer: -1.5 ± 0.9 l/min) compared with thermodilution (-3.8 ± 1.19 l/min). These results demonstrate that the Modelflow method, regardless of Finometer or direct arterial waveforms, underestimates cardiac output during heat stress and during subsequent reductions in cardiac output via LBNP.
Figures



References
-
- Cui J, Wilson TE, Crandall CG. Phenylephrine-induced elevations in arterial blood pressure are attenuated in heat-stressed humans. Am J Physiol Regul Integr Comp Physiol 283:R1221–R1226, 2002 - PubMed
-
- Dyson KS, Shoemaker JK, Arbeille P, Hughson RL. Modelflow estimates of cardiac output compared with Doppler ultrasound during acute changes in vascular resistance in women. Exp Physiol 95:561–568, 2010 - PubMed
-
- Harms MP, Wesseling KH, Pott F, Jenstrup M, Van Goudoever J, Secher NH, Van Lieshout JJ. Continuous stroke volume monitoring by modelling flow from non-invasive measurement of arterial pressure in humans under orthostatic stress. Clin Sci (Lond) 97:291–301, 1999 - PubMed
-
- Heerman JR, Segers P, Roosens CD, Gasthuys F, Verdonck PR, Poelaert JI. Echocardiographic assessment of aortic elastic properties with automated border detection in an ICU: in vivo application of the arctangent Langewouters model. Am J Physiol Heart Circ Physiol 288:H2504–H2511, 2005 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical