

The effects of age on inflammatory and coagulation-fibrinolysis response in patients hospitalized for pneumonia
- PMID: 21085465
- PMCID: PMC2973976
- DOI: 10.1371/journal.pone.0013852
The effects of age on inflammatory and coagulation-fibrinolysis response in patients hospitalized for pneumonia
Abstract
Objective: To determine whether inflammatory and hemostasis response in patients hospitalized for pneumonia varies by age and whether these differences explain higher mortality in the elderly.
Methods: In an observational cohort of subjects with community-acquired pneumonia (CAP) recruited from emergency departments (ED) in 28 hospitals, we divided subjects into 5 age groups (<50, 51-64, 65-74, 75-84, and ≥85). We measured circulating levels of inflammatory (TNF, IL-6, and IL-10), hemostasis (D-dimer, Factor IX, thrombin-antithrombin complex, antithrombin and plasminogen-activator inhibitor-1), and cell-surface markers (TLR-2, TLR-4, and HLA-DR) during the first week of hospitalization and at discharge and compared 90-day mortality. We used logistic regression to compare odds ratios (OR) for 90-day mortality between age groups, adjusting for differences in pre-infection factors alone and then additionally adjusting for immune markers.
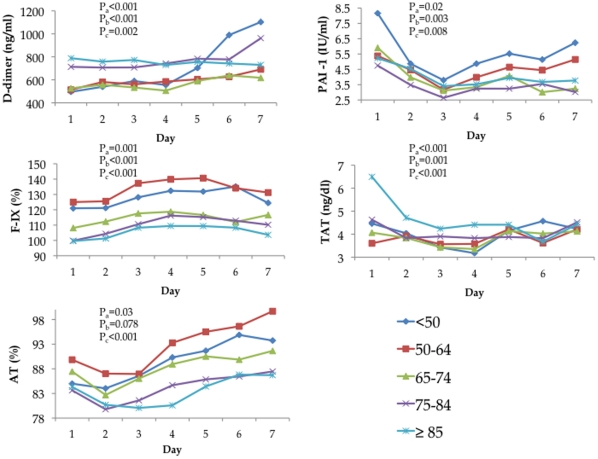
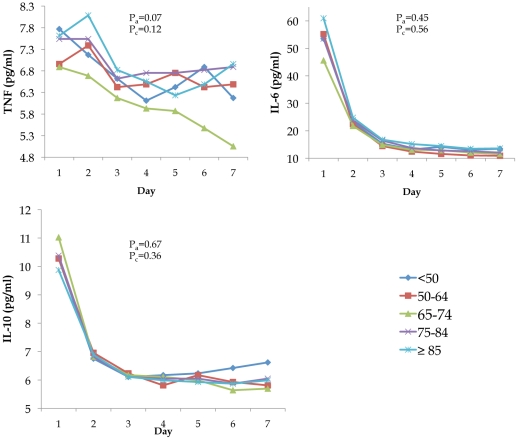
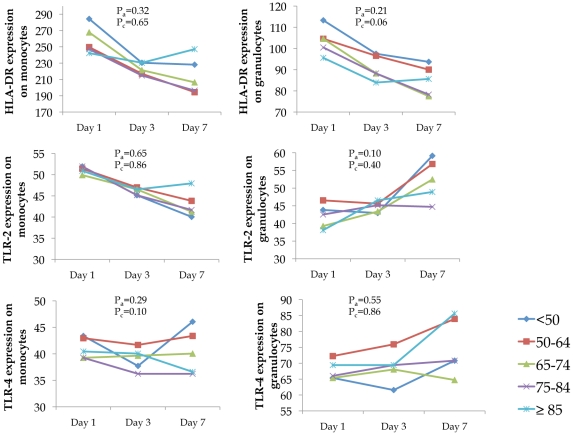
Results: Of 2,183 subjects, 495, 444, 403, 583, and 258 subjects were <50, 51-64, 65-74, 75-84, and ≥85 years of age, respectively. Large age-related differences were observed in 90-day mortality (0.82% vs. 3.2% vs. 6.4% vs. 12.8% vs. 13.6%, p<0.01). No age-related differences in inflammatory and cell surface markers occurred during the first week. Older subjects had higher pro-coagulant markers on ED presentation and over first week (p ≤ 0.03), but these differences were modest (1.0-1.7-fold differences). Odds of death for older adults changed minimally in models incorporating differences in hemostasis and inflammatory markers (for subjects ≥ 85 compared to those <50, OR = 4.36, when adjusted for pre-infection factors and OR = 3.49 when additionally adjusted for hemostasis markers). At discharge, despite clinical recovery as evidenced by normal vital signs in >85% subjects, older subjects had modestly increased hemostasis markers and IL-6 levels (p<0.01).
Conclusions: Modest age-related increases in coagulation response occur during hospitalization for CAP; however these differences do not explain the large differences in mortality. Despite clinical recovery, immune resolution may be delayed in older adults at discharge.
Conflict of interest statement
Figures
References
-
- Angus DC, Linde-Zwirble WT, Lidicker J, Clermont G, Carcillo J, et al. Epidemiology of severe sepsis in the United States: analysis of incidence, outcome, and associated costs of care. Crit Care Med. 2001;29:1303–1310. - PubMed
-
- Martin GS, Mannino DM, Moss M. The effect of age on the development and outcome of adult sepsis. Crit Care Med. 2006;34:15–21. - PubMed
-
- Kaplan V, Angus DC, Griffin MF, Clermont G, Scott Watson R, et al. Hospitalized community-acquired pneumonia in the elderly: age- and sex-related patterns of care and outcome in the United States. Am J Respir Crit Care Med. 2002;165:766–772. - PubMed
-
- Girard TD, Ely EW. Bacteremia and sepsis in older adults. Clin Geriatr Med. 2007;23:633–647, viii. - PubMed
-
- Waterer GW, Kessler LA, Wunderink RG. Medium-term survival after hospitalization with community-acquired pneumonia. Am J Respir Crit Care Med. 2004;169:910–914. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
