

BMI, all-cause and cause-specific mortality in Chinese Singaporean men and women: the Singapore Chinese health study
- PMID: 21085577
- PMCID: PMC2981556
- DOI: 10.1371/journal.pone.0014000
BMI, all-cause and cause-specific mortality in Chinese Singaporean men and women: the Singapore Chinese health study
Abstract
Background: The optimal range of relative weight for morbidity and mortality in Asian populations is an important question in need of more thorough investigation, especially as obesity rates increase. We aimed to examine the association between body mass index (BMI), all cause and cause-specific mortality to determine the optimal range of BMI in relation to mortality in Chinese men and women in Singapore.
Methodology/principal findings: We analyzed data from a prospective cohort study of 51,251 middle-aged or older (45-74) Chinese men and women in the Singapore Chinese Health Study. Participants were enrolled and data on body weight and covariates were collected in 1993-1998 and participants were followed through 2008. The analysis accounted for potential methodological issues through stratification on smoking and age, thorough adjustment of demographic and lifestyle confounders and exclusion of deaths early in the follow-up.
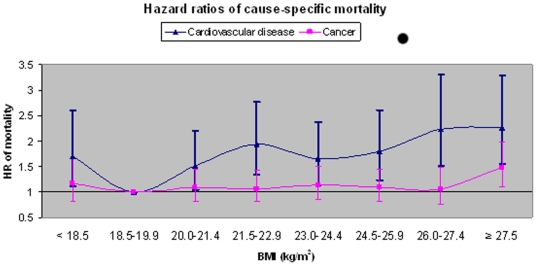
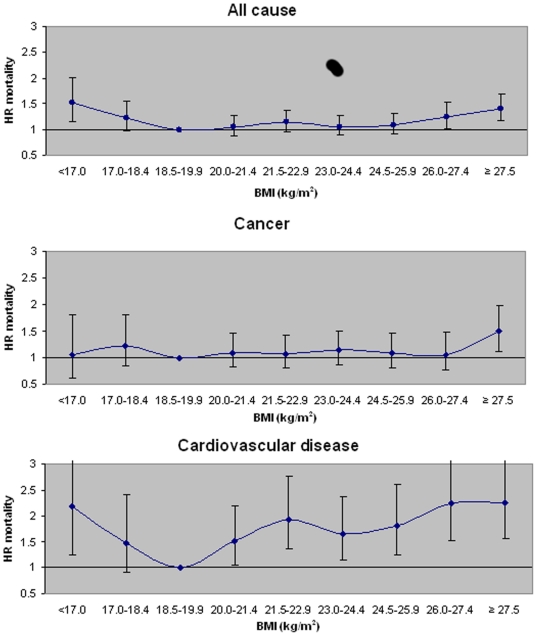
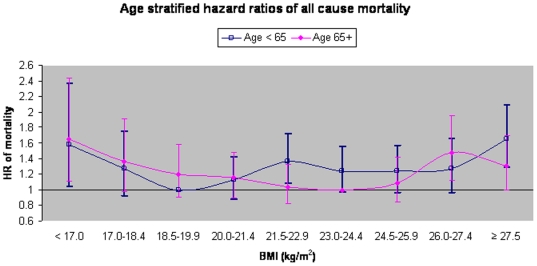
Conclusions/significance: Increased risk of mortality was apparent in underweight (<18.5) and obese BMI categories (≥27.5) independent of age and smoking. Regardless of age or BMI, smoking considerably increased the rate of mortality and modified the association between BMI and mortality. The most favorable range of BMI for mortality rates and risk in non-smoking persons below age 65 was 18.5-21.4 kg/m(2), and for non-smoking persons aged 65 and above was 21.5-24.4 kg/m(2).
Conflict of interest statement
Figures
References
-
- Yoon KH, Lee JH, Kim JW, Cho JH, Choi YH, et al. Epidemic obesity and type 2 diabetes in Asia. Lancet. 2006;368:1681–8. - PubMed
-
- Fontaine K, Allison DB. Obesity and Mortality Rates. In: Bray GA, editor. in Handbook of Obesity: Etiology and Pathophysiology. New York: Marcel Dekker; 2004. pp. 767–785.
-
- Yuan J, Ross RK, Gao YT, Yu MC. Body weight and mortality: a prospective evaluation in a cohort of middle-aged men in Shanghai, China. Int J Epidem. 1998;27:824–832. - PubMed
-
- Tsugane S, Sasaki S, Tsubono Y. Under-and overweight impact on mortality among middle-aged Japanese men and women: a 10-y follow-up of JPHC study cohort I. Int J Obes. 2002;26:529–537. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
