

Anatomy of the lateral ligaments of the rectum: a controversial point of view
- PMID: 21086557
- PMCID: PMC2988232
- DOI: 10.3748/wjg.v16.i43.5411
Anatomy of the lateral ligaments of the rectum: a controversial point of view
Abstract
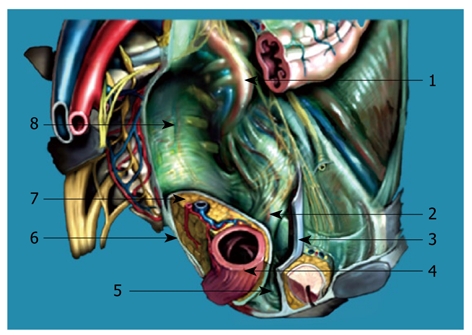
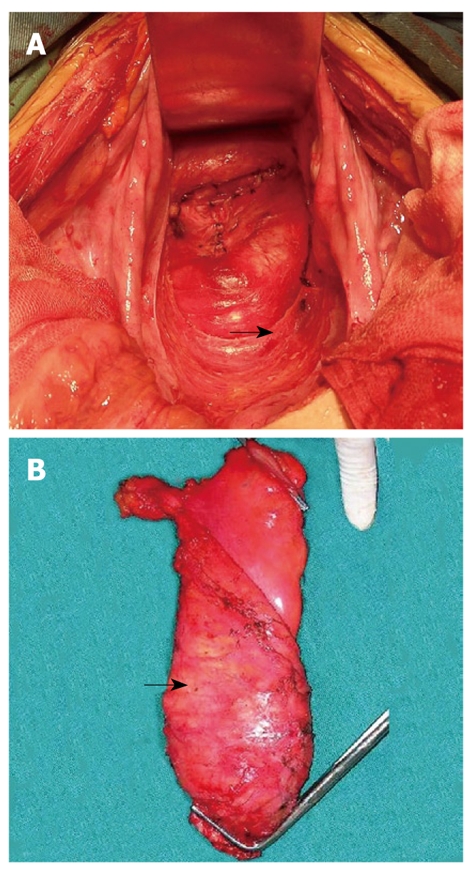
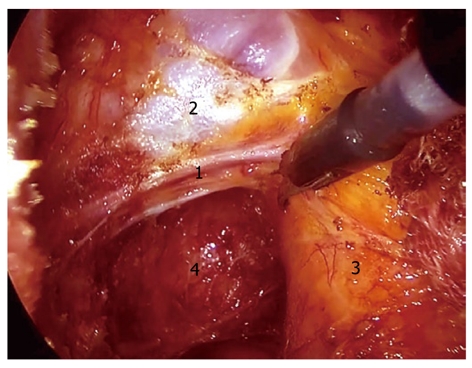
The existence and composition of the lateral ligaments of the rectum (LLR) are still the subjects of anatomical confusion and surgical misconception up to now. Since Miles proposed abdominoperineal excision as radical surgery for rectal cancer, the identification by "hooking them on the finger" has been accepted by many surgeons with no doubt; clamping, dividing and ligating are considered to be essential procedures in mobilization of the rectum in many surgical textbooks. But in cadaveric studies, many anatomists could not find LLR described by the textbooks, and more and more surgeons also failed to find LLR during the proctectomy according to the principle of total mesorectal excision. The anatomy of LLR has diverse descriptions in literatures. According to our clinical observations, the traditional anatomical structures of LLR do exist; LLR are constant dense connective bundles which are located in either lateral side of the lower part of the rectum, run between rectal visceral fascia and pelvic parietal fascia above the levator ani, and covered by superior fascia of pelvic diaphragm. They are pathways of blood vessels and nerve fibers toward the rectum and lymphatic vessels from the lower rectum toward the iliac lymph nodes.
Figures
Similar articles
-
Lateral ligaments of the rectum: an anatomical study.Br J Surg. 1999 Apr;86(4):487-9. doi: 10.1046/j.1365-2168.1999.01080.x. Br J Surg. 1999. PMID: 10215819
-
The anatomy of lateral ligament of the rectum and its role in total mesorectal excision.World J Surg. 2010 Mar;34(3):594-8. doi: 10.1007/s00268-009-0371-1. World J Surg. 2010. PMID: 20052469
-
The vascular and neuronal composition of the lateral ligament of the rectum and the rectosacral fascia.Surg Radiol Anat. 1991;13(1):17-22. doi: 10.1007/BF01623135. Surg Radiol Anat. 1991. PMID: 2053040
-
Lateral ligament: its anatomy and clinical importance.Semin Surg Oncol. 2000 Dec;19(4):386-95. doi: 10.1002/ssu.9. Semin Surg Oncol. 2000. PMID: 11241921 Review.
-
The characteristics of the urogenital fascia in the retrorectal space based on male cadaveric dissection and its clinical application.BMC Surg. 2023 Apr 17;23(1):93. doi: 10.1186/s12893-023-01993-w. BMC Surg. 2023. PMID: 37069543 Free PMC article. Review.
Cited by
-
Neuro-anatomy of the posterior parametrium and surgical considerations for a nerve-sparing approach in radical pelvic surgery.Surg Endosc. 2013 Nov;27(11):4386-94. doi: 10.1007/s00464-013-3043-z. Epub 2013 Jun 20. Surg Endosc. 2013. PMID: 23783554
-
Radical Hysterectomy or Total Mesometrial Resection-Two Anatomical Concepts for Surgical Treatment of Cancer of the Uterine Cervix.Cancers (Basel). 2023 Nov 5;15(21):5295. doi: 10.3390/cancers15215295. Cancers (Basel). 2023. PMID: 37958469 Free PMC article. Review.
-
Exposure of the Middle Rectal Artery and Lateral Ligament of the Rectum Following the Gate Approach during Total Mesorectal Excision.Yonsei Med J. 2022 May;63(5):490-492. doi: 10.3349/ymj.2022.63.5.490. Yonsei Med J. 2022. PMID: 35512752 Free PMC article.
-
The Mesentery in Robot-Assisted Total Mesorectal Excision.Clin Colon Rectal Surg. 2022 Aug 10;35(4):298-305. doi: 10.1055/s-0042-1743583. eCollection 2022 Jul. Clin Colon Rectal Surg. 2022. PMID: 35975108 Free PMC article. Review.
-
Urinary and sexual dysfunction rates and risk factors following rectal cancer surgery.Int J Colorectal Dis. 2015 Nov;30(11):1547-55. doi: 10.1007/s00384-015-2346-z. Epub 2015 Aug 13. Int J Colorectal Dis. 2015. PMID: 26264048
References
-
- Gaudio E, Riva A, Franchitto A, Carpino G. The fascial structures of the rectum and the "so-called mesorectum": an anatomical or a terminological controversy? Surg Radiol Anat. 2010;32:189–190. - PubMed
-
- Koura AN, Giacco GG, Curley SA, Skibber JM, Feig BW, Ellis LM. Carcinoid tumors of the rectum: effect of size, histopathology, and surgical treatment on metastasis free survival. Cancer. 1997;79:1294–1298. - PubMed
-
- Heald RJ, Smedh RK, Kald A, Sexton R, Moran BJ. Abdominoperineal excision of the rectum--an endangered operation. Norman Nigro Lectureship. Dis Colon Rectum. 1997;40:747–751. - PubMed
-
- da Silva AL. Abdominoperineal excision of the rectum and anal canal with perineal colostomy. Eur J Surg. 1995;161:761–764. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
