

Predictors of rebleeding after initial hemostasis with epinephrine injection in high-risk ulcers
- PMID: 21086569
- PMCID: PMC2988244
- DOI: 10.3748/wjg.v16.i43.5490
Predictors of rebleeding after initial hemostasis with epinephrine injection in high-risk ulcers
Abstract
Aim: To identify the predictors of rebleeding after initial hemostasis with epinephrine injection (EI) in patients with high-risk ulcers.
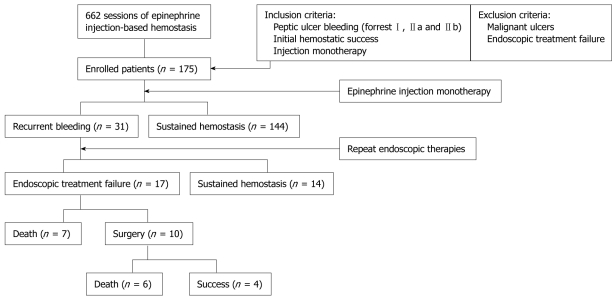
Methods: Recent studies have revealed that endoscopic thermocoagulation, or clips alone or combined with EI are superior to EI alone to arrest ulcer bleeding. However, the reality is that EI monotherapy is still common in clinical practice. From October 2006 to April 2008, high-risk ulcer patients in whom hemorrhage was stopped after EI monotherapy were studied using clinical, laboratory and endoscopic variables. The patients were divided into 2 groups: sustained hemostasis and rebleeding.
Results: A total of 175 patients (144, sustained hemostasis; 31, rebleeding) were enrolled. Univariate analysis revealed that older age (≥ 60 years), advanced American Society of Anesthesiology (ASA) status (category III, IV and V), shock, severe anemia (hemoglobin < 80 g/L), EI dose ≥ 12 mL and severe bleeding signs (SBS) including hematemesis or hematochezia were the factors which predicted rebleeding. However, only older age, severe anemia, high EI dose and SBS were independent predictors. Among 31 rebleeding patients, 10 (32.2%) underwent surgical hemostasis, 15 (48.4%) suffered from delayed hemostasis causing major complications and 13 (41.9%) died of these complications.
Conclusion: Endoscopic EI monotherapy in patients with high-risk ulcers should be avoided. Initial hemostasis with thermocoagulation, clips or additional hemostasis after EI is mandatory for such patients to ensure better hemostatic status and to prevent subsequent rebleeding, surgery, morbidity and mortality.
Figures
References
-
- Church NI, Palmer KR. Ulcers and nonvariceal bleeding. Endoscopy. 2003;35:22–26. - PubMed
-
- Sugawa C, Joseph AL. Endoscopic interventional management of bleeding duodenal and gastric ulcers. Surg Clin North Am. 1992;72:317–334. - PubMed
-
- Villanueva C, Balanzó J, Espinós JC, Fábrega E, Sáinz S, González D, Vilardell F. Endoscopic injection therapy of bleeding ulcer: a prospective and randomized comparison of adrenaline alone or with polidocanol. J Clin Gastroenterol. 1993;17:195–200. - PubMed
-
- Consensus conference: Therapeutic endoscopy and bleeding ulcers. JAMA. 1989;262:1369–1372. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Miscellaneous
