

From singing to speaking: facilitating recovery from nonfluent aphasia
- PMID: 21088709
- PMCID: PMC2982746
- DOI: 10.2217/fnl.10.44
From singing to speaking: facilitating recovery from nonfluent aphasia
Abstract
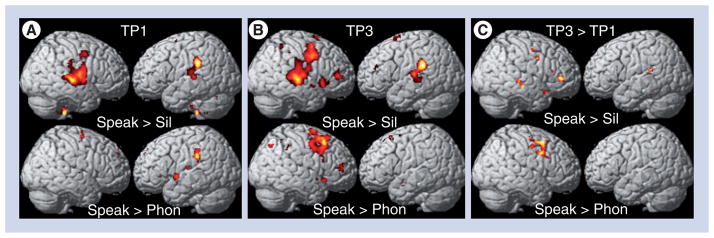
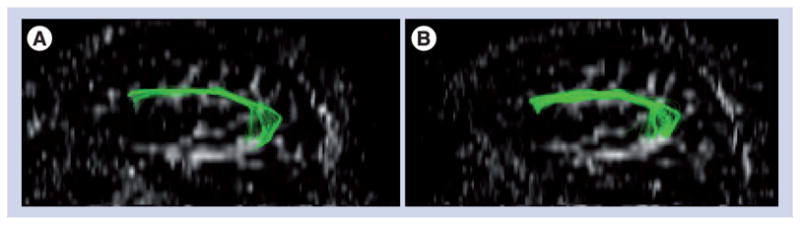
It has been reported for more than 100 years that patients with severe nonfluent aphasia are better at singing lyrics than they are at speaking the same words. This observation led to the development of melodic intonation therapy (MIT). However, the efficacy of this therapy has yet to be substantiated in a randomized controlled trial. Furthermore, its underlying neural mechanisms remain unclear. The two unique components of MIT are the intonation of words and simple phrases using a melodic contour that follows the prosody of speech and the rhythmic tapping of the left hand that accompanies the production of each syllable and serves as a catalyst for fluency. Research has shown that both components are capable of engaging fronto-temporal regions in the right hemisphere, thereby making MIT particularly well suited for patients with large left hemisphere lesions who also suffer from nonfluent aphasia. Recovery from aphasia can happen in two ways: either through the recruitment of perilesional brain regions in the affected hemisphere, with variable recruitment of right-hemispheric regions if the lesion is small, or through the recruitment of homologous language and speech-motor regions in the unaffected hemisphere if the lesion of the affected hemisphere is extensive. Treatment-associated neural changes in patients undergoing MIT indicate that the unique engagement of right-hemispheric structures (e.g., the superior temporal lobe, primary sensorimotor, premotor and inferior frontal gyrus regions) and changes in the connections across these brain regions may be responsible for its therapeutic effect.
Figures
References
Bibliography
-
- Pedersen PM, Jorgensen HS, Nakayama H, Raaschou HO, Olsen TS. Aphasia in acute stroke: incidence, determinants, and recovery. Ann Neurol. 1995;38:659–666. - PubMed
-
- Pedersen PM, Vinter K, Olsen TS. Aphasia after stroke: type, severity and prognosis The Copenhagen aphasia study. Cerebrovasc Dis. 2004;17(1):35–43. - PubMed
-
- Kertesz A, McCabe P. Recovery patterns and prognosis in aphasia. Brain. 1977;100(Pt 1):1–18. - PubMed
-
- Kertesz A, Lesk D, McCabe P. Isotope localization of infarcts in aphasia. Arch Neurol. 1977;34(10):590–601. - PubMed
Websites
-
- The National Aphasia Society. www.aphasia.org/Aphasia%20Facts/aphasia_faq.html.
-
- Music, Neuroimaging and Stroke Recovery Laboratories. www.musicianbrain.com/#aphasia.
-
- Melodic intonation therapy and speech repetition therapy for patients with nonfluent aphasia. http://clinicaltrials.gov/ct2/show/NCT00903266?term=Melodic+Intonation+T....
Grants and funding
LinkOut - more resources
Full Text Sources