

Pericardial approach for cardiac therapies: old practice with new ideas
- PMID: 21088750
- PMCID: PMC2978289
- DOI: 10.4070/kcj.2010.40.10.479
Pericardial approach for cardiac therapies: old practice with new ideas
Abstract
Treatment of cardiac disease via the epicardium fell under the domain of cardiac surgery due to the need for an open thoracotomy. Since an open thoracotomy is invasive in nature and has the potential for complications, a minimally invasive and percutaneous approach would be more attractive for suitable patients. The recent success of epicardial ablation of refractory arrhythmia via the percutaneous pericardial approach has increased the potential for delivery of epicardial therapies. Epicardial ablation has increased the success and safety since anti-coagulation and transseptal catheterization for left atrial arrhythmias is not required. The pericardial space has also been used to deliver therapy for several cardiac diseases. There are reports on successful delivery of drugs and their efficacy. Even though there was a wide range of efficacies reported in those studies, the reported complication rates are strikingly low, which suggests that direct delivery of drugs to the epicardium via the pericardial space is safe. Furthermore, recent animal studies have supported the feasibility of epicardial delivery of biological agents, including genes, cells, and even genetically engineered tissue for therapeutic purposes. In conclusion, percutaneous pericardial cannulation of closed pericardial space can play a significant role in providing non-surgical therapy for cardiovascular diseases. However, it requires skills and operator experiences. Therefore, there is need to further develop new tools, safer techniques, and effective procedure environment before generalizing this procedure.
Keywords: Administration routes, drug; Cannulation; Pericardium.
Figures
Similar articles
-
Subxiphoid surgical approach for epicardial catheter-based mapping and ablation in patients with prior cardiac surgery or difficult pericardial access.Circulation. 2004 Sep 7;110(10):1197-201. doi: 10.1161/01.CIR.0000140725.42845.90. Epub 2004 Aug 30. Circulation. 2004. PMID: 15337702
-
Surgical pericardial adhesions do not preclude minimally invasive epicardial pacemaker lead placement in an infant porcine model.J Cardiovasc Electrophysiol. 2020 Nov;31(11):2975-2981. doi: 10.1111/jce.14724. Epub 2020 Aug 31. J Cardiovasc Electrophysiol. 2020. PMID: 32841456
-
The effectiveness of rigid pericardial endoscopy for minimally invasive minor surgeries: cell transplantation, epicardial pacemaker lead implantation, and epicardial ablation.J Cardiothorac Surg. 2012 Nov 9;7:117. doi: 10.1186/1749-8090-7-117. J Cardiothorac Surg. 2012. PMID: 23140449 Free PMC article.
-
Transthoracic epicardial catheter ablation: indications, techniques, and complications.Circ J. 2013;77(7):1672-80. doi: 10.1253/circj.cj-13-0510. Epub 2013 Jun 12. Circ J. 2013. PMID: 23759656 Review.
-
The Future of Percutaneous Epicardial Interventions.Card Electrophysiol Clin. 2020 Sep;12(3):419-430. doi: 10.1016/j.ccep.2020.04.007. Epub 2020 Jul 1. Card Electrophysiol Clin. 2020. PMID: 32771195 Review.
Cited by
-
Evaluation of upconverting nanoparticles towards heart theranostics.PLoS One. 2019 Dec 9;14(12):e0225729. doi: 10.1371/journal.pone.0225729. eCollection 2019. PLoS One. 2019. PMID: 31815963 Free PMC article.
-
Current Landscape of Gene Therapy for the Treatment of Cardiovascular Disorders.Curr Gene Ther. 2024;24(5):356-376. doi: 10.2174/0115665232268840231222035423. Curr Gene Ther. 2024. PMID: 38288826 Review.
References
-
- Sosa E, Scanavacca M, d'Avila A, Pilleggi F. A new technique to perform epicardial mapping in the electrophysiology laboratory. J Cardiovasc Electrophysiol. 1996;7:531–536. - PubMed
-
- Maisch B, Karatolios K. New possibilities of diagnostics and therapy of pericarditis. Internist (Berl) 2008;49:17–26. - PubMed
-
- Braunwald E, Libby P. Braunwald's Heart Disease: A Textbook of Cardiovascular Medicine. 7 ed. Philadelphia: Saunders; 2007.
-
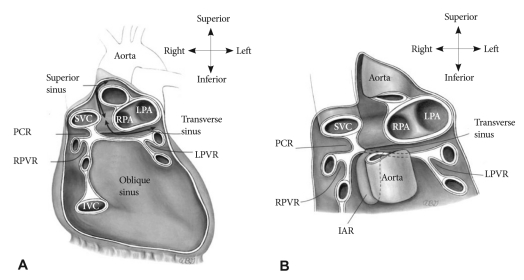
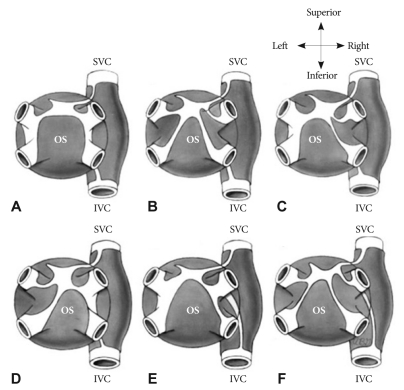
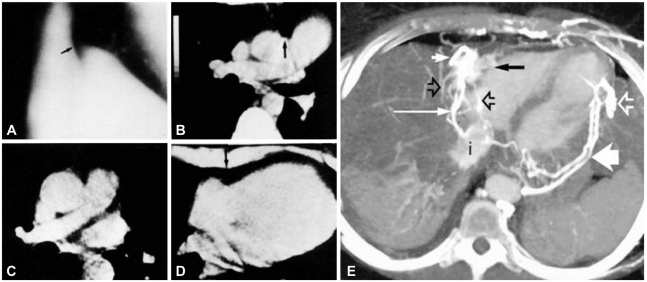
- Choe YH, Im JG, Park JH, Han MC, Kim CW. The anatomy of the pericardial space: a study in cadavers and patients. AJR Am J Roentgenol. 1987;149:693–697. - PubMed
-
- Groell R, Schaffler GJ, Rienmueller R. Pericardial sinuses and recesses: findings at electrocardiographically triggered electron-beam CT. Radiology. 1999;212:69–73. - PubMed
LinkOut - more resources
Full Text Sources
