

Toward fulfilling the promise of molecular medicine in fragile X syndrome
- PMID: 21090964
- PMCID: PMC3100156
- DOI: 10.1146/annurev-med-061109-134644
Toward fulfilling the promise of molecular medicine in fragile X syndrome
Abstract
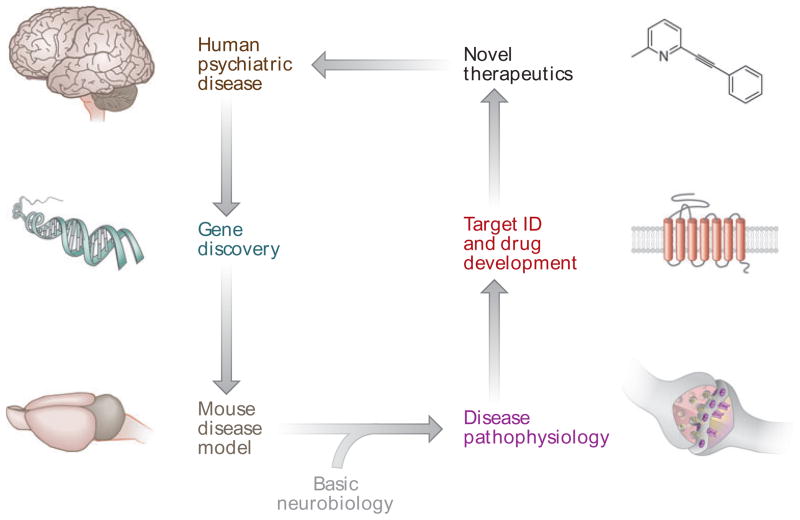
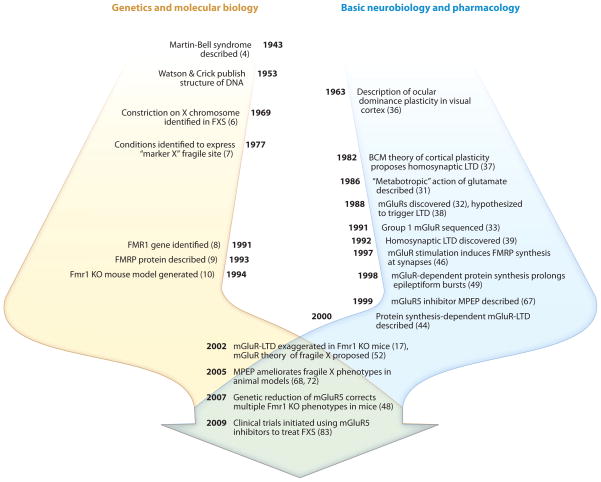
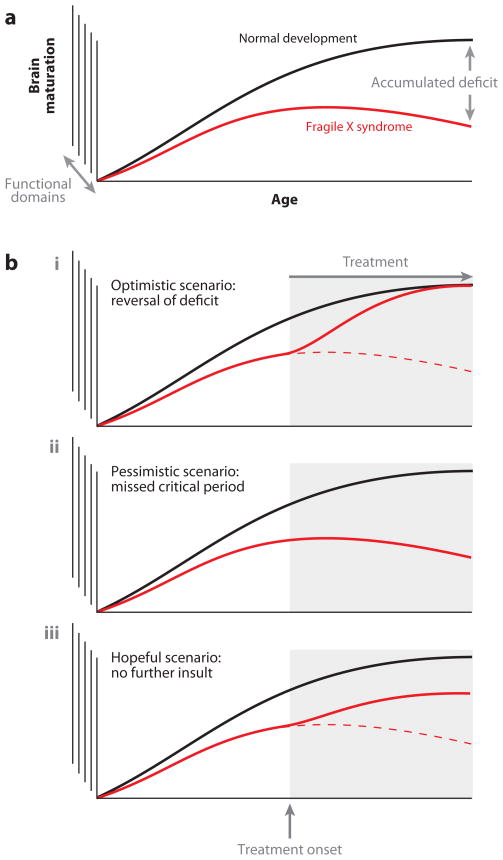
Fragile X syndrome (FXS) is the most common inherited form of mental retardation and a leading known cause of autism. It is caused by loss of expression of the fragile X mental retardation protein (FMRP), an RNA-binding protein that negatively regulates protein synthesis. In neurons, multiple lines of evidence suggest that protein synthesis at synapses is triggered by activation of group 1 metabotropic glutamate receptors (Gp1 mGluRs) and that many functional consequences of activating these receptors are altered in the absence of FMRP. These observations have led to the theory that exaggerated protein synthesis downstream of Gp1 mGluRs is a core pathogenic mechanism in FXS. This excess can be corrected by reducing signaling by Gp1 mGluRs, and numerous studies have shown that inhibition of mGluR5, in particular, can ameliorate multiple mutant phenotypes in animal models of FXS. Clinical trials based on this therapeutic strategy are currently under way. FXS is therefore poised to be the first neurobehavioral disorder in which corrective treatments have been developed from the bottom up: from gene identification to pathophysiology in animals to novel therapeutics in humans. The insights gained from FXS and other autism-related single-gene disorders may also assist in identifying molecular mechanisms and potential treatment approaches for idiopathic autism.
Figures
References
-
- Hyman SE. The role of molecular biology in psychiatry. Psychosomatics. 1988;29:328–32. - PubMed
-
- Kogan MD, Blumberg SJ, Schieve LA, et al. Prevalence of parent-reported diagnosis of autism spectrum disorder among children in the US, 2007. Pediatrics. 2009;124:1395–403. - PubMed
-
- Penagarikano O, Mulle JG, Warren ST. The pathophysiology of fragile X syndrome. Annu Rev Genomics Hum Genet. 2007;8:109–29. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
