

In-center hemodialysis six times per week versus three times per week
- PMID: 21091062
- PMCID: PMC3042140
- DOI: 10.1056/NEJMoa1001593
In-center hemodialysis six times per week versus three times per week
Erratum in
- N Engl J Med. 2011 Jan 6;364(1):93
Abstract
Background: In this randomized clinical trial, we aimed to determine whether increasing the frequency of in-center hemodialysis would result in beneficial changes in left ventricular mass, self-reported physical health, and other intermediate outcomes among patients undergoing maintenance hemodialysis.
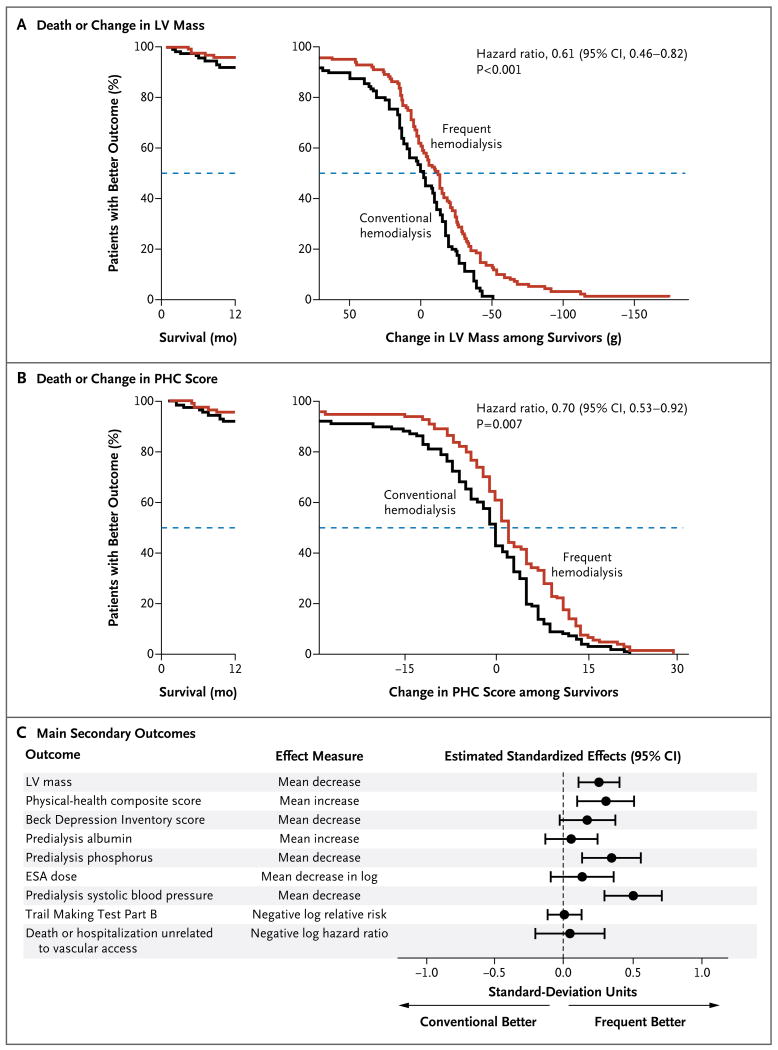
Methods: Patients were randomly assigned to undergo hemodialysis six times per week (frequent hemodialysis, 125 patients) or three times per week (conventional hemodialysis, 120 patients) for 12 months. The two coprimary composite outcomes were death or change (from baseline to 12 months) in left ventricular mass, as assessed by cardiac magnetic resonance imaging, and death or change in the physical-health composite score of the RAND 36-item health survey. Secondary outcomes included cognitive performance; self-reported depression; laboratory markers of nutrition, mineral metabolism, and anemia; blood pressure; and rates of hospitalization and of interventions related to vascular access.
Results: Patients in the frequent-hemodialysis group averaged 5.2 sessions per week; the weekly standard Kt/V(urea) (the product of the urea clearance and the duration of the dialysis session normalized to the volume of distribution of urea) was significantly higher in the frequent-hemodialysis group than in the conventional-hemodialysis group (3.54±0.56 vs. 2.49±0.27). Frequent hemodialysis was associated with significant benefits with respect to both coprimary composite outcomes (hazard ratio for death or increase in left ventricular mass, 0.61; 95% confidence interval [CI], 0.46 to 0.82; hazard ratio for death or a decrease in the physical-health composite score, 0.70; 95% CI, 0.53 to 0.92). Patients randomly assigned to frequent hemodialysis were more likely to undergo interventions related to vascular access than were patients assigned to conventional hemodialysis (hazard ratio, 1.71; 95% CI, 1.08 to 2.73). Frequent hemodialysis was associated with improved control of hypertension and hyperphosphatemia. There were no significant effects of frequent hemodialysis on cognitive performance, self-reported depression, serum albumin concentration, or use of erythropoiesis-stimulating agents.
Conclusions: Frequent hemodialysis, as compared with conventional hemodialysis, was associated with favorable results with respect to the composite outcomes of death or change in left ventricular mass and death or change in a physical-health composite score but prompted more frequent interventions related to vascular access. (Funded by the National Institute of Diabetes and Digestive and Kidney Diseases and others; ClinicalTrials.gov number, NCT00264758.).
Figures
Comment in
-
"Daily" dialysis--lessons from a randomized, controlled trial.N Engl J Med. 2010 Dec 9;363(24):2363-4. doi: 10.1056/NEJMe1012205. Epub 2010 Nov 20. N Engl J Med. 2010. PMID: 21091061 No abstract available.
-
Dialysis: High-frequency dialysis offers clear benefits—but at what cost?Nat Rev Nephrol. 2011 Feb;7(2):61. doi: 10.1038/nrneph.2010.180. Nat Rev Nephrol. 2011. PMID: 21355119 No abstract available.
-
Frequent versus standard hemodialysis.N Engl J Med. 2011 Mar 10;364(10):975-6; author reply 976. doi: 10.1056/NEJMc1100105. N Engl J Med. 2011. PMID: 21388318 No abstract available.
-
Frequent versus standard hemodialysis.N Engl J Med. 2011 Mar 10;364(10):975; author reply 976. doi: 10.1056/NEJMc1100105. N Engl J Med. 2011. PMID: 21388319 No abstract available.
-
Frequent versus standard hemodialysis.N Engl J Med. 2011 Mar 10;364(10):974-5; author reply 976. doi: 10.1056/NEJMc1100105. N Engl J Med. 2011. PMID: 21388320 No abstract available.
-
Frequent versus standard hemodialysis.N Engl J Med. 2011 Mar 10;364(10):974; author reply 976. doi: 10.1056/NEJMc1100105. N Engl J Med. 2011. PMID: 21388321 No abstract available.
-
ACP Journal Club. Increased frequency of hemodialysis reduced adverse clinical outcomes.Ann Intern Med. 2011 Apr 19;154(8):JC4-6. doi: 10.7326/0003-4819-154-8-201104190-02006. Ann Intern Med. 2011. PMID: 21502644 No abstract available.
-
Time to move to more frequent haemodialysis?Natl Med J India. 2011 Mar-Apr;24(2):91-3. Natl Med J India. 2011. PMID: 21668054 No abstract available.
References
-
- Renal Data System . USRDS 2009 annual data report: atlas of chronic kidney disease and end-stage renal disease in the United States. Bethesda, MD: National Institute of Diabetes and Digestive and Kidney Diseases; 2009. http://www.usrds.org.
-
- Scribner BH, Buri R, Caner JE, Hegstrom R, Burnell JM. The treatment of chronic uremia by means of intermittent hemodialysis: a preliminary report. Trans Am Soc Artif Intern Organs. 1960;6:114–22. - PubMed
-
- Teschan PE, Ginn HE, Bourne JR, Walker PJ, Ward JW. Quantitative neurobehavioral responses to renal failure and maintenance dialysis. Trans Am Soc Artif Intern Organs. 1975;21:488–91. - PubMed
-
- Held PJ, Pauly MV. Competition and efficiency in the End-Stage Renal Disease program. J Health Econ. 1983;2:95–118. - PubMed
-
- Evans RW, Manninen DL, Garrison LP, Jr, et al. The quality of life of patients with end-stage renal disease. N Engl J Med. 1985;312:553–9. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical