

Genetically modified donor leukocyte transfusion and graft-versus-leukemia effect after allogeneic stem cell transplantation
- PMID: 21091264
- PMCID: PMC3135250
- DOI: 10.1089/hum.2010.162
Genetically modified donor leukocyte transfusion and graft-versus-leukemia effect after allogeneic stem cell transplantation
Abstract
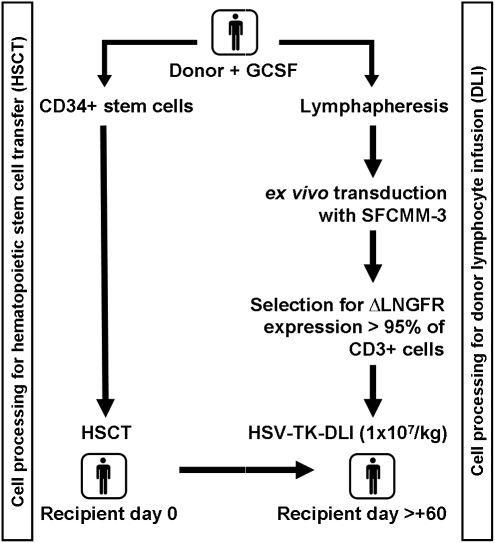
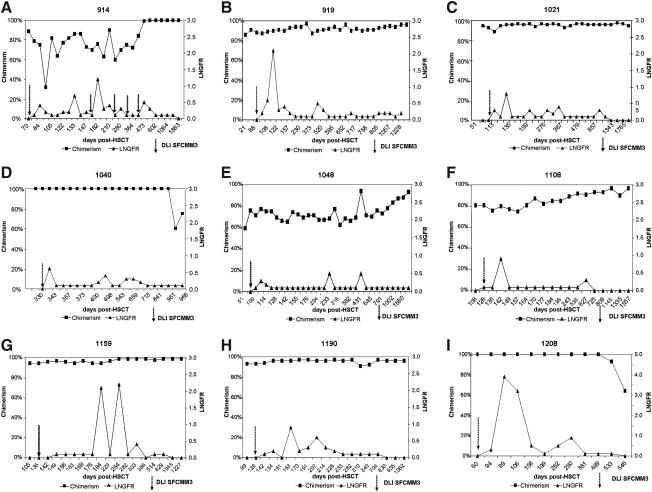
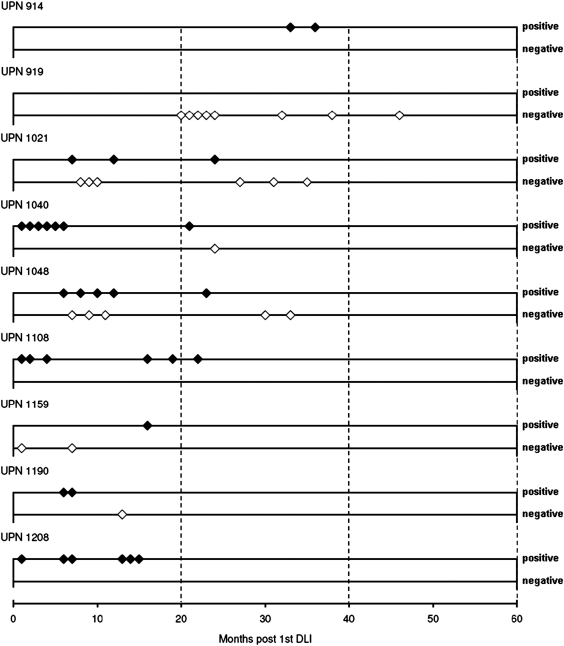
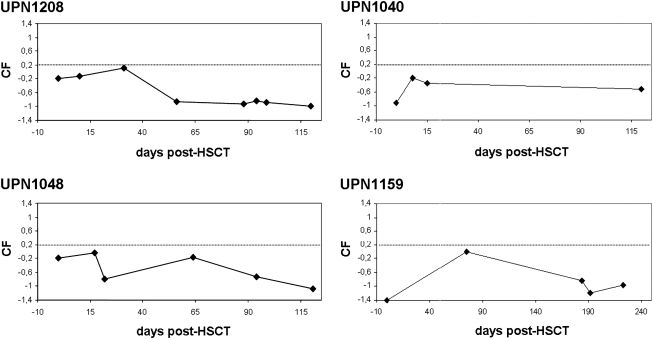
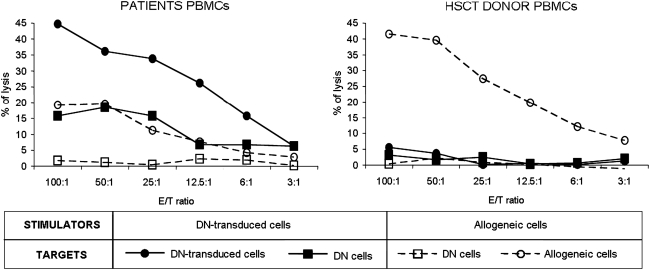
Seven patients with acute myeloid leukemia (AML) and two patients with chronic myelogenous leukemia (CML) were transplanted from HLA-identical sibling donors with CD34(+) cell-enriched stem cells (HSCTs) without further immunosuppression. The myeloablative standard transplantation protocol was adapted to include transfusion of gene-modified donor T cells after HSCT. Donor T cells were transduced with the replication-deficient retrovirus SFCMM-3, which expresses herpes simplex thymidine kinase (HSV-Tk) and a truncated version of low-affinity nerve growth factor receptor (ΔLNGFR) for selection and characterization of transduced cells. Transduced T cells were detectable in all patients during follow-up for up to 5 years after transfusion. Proteomic screening for development of acute graft-versus-host disease (aGvHD) was applied to five of the seven patients with AML. No positivity for the aGvHD grade II-specific proteomic pattern was observed. Only one patient developed aGvHD grade I. To date, three of the patients with AML relapsed; one responded to three escalating transfusions of lymphocytes from the original donor and is in complete remission. Two were retransplanted with non-T cell-depleted peripheral blood stem cells from their original donors and died after retransplantation of septic complications or relapse, respectively. In one patient with CML, loss of bcr-abl gene expression was observed after an expansion of transduced cells. Seven of nine patients are alive and in complete remission.
Figures
References
-
- Bahceci E. Epperson D. Douek D.C., et al. Early reconstitution of the T-cell repertoire after non-myeloablative peripheral blood stem cell transplantation is from post-thymic T-cell expansion and is unaffected by graft-versus-host disease or mixed chimaerism. Br. J. Haematol. 2003;122:934–943. - PubMed
-
- Barrett A.J. Mavroudis D. Tisdale J., et al. T cell-depleted bone marrow transplantation and delayed T cell add-back to control acute GVHD and conserve a graft-versus-leukemia effect. Bone Marrow Transplant. 1998;21:543–551. - PubMed
-
- Bondanza A. Valtolina V. Magnani Z., et al. Suicide gene therapy of graft-versus-host disease induced by central memory human T lymphocytes. Blood. 2006;107:1828–1836. - PubMed
-
- Bonini C. Ciceri F. Marktel S., et al. Suicide-gene-transduced T-cells for the regulation of the graft-versus-leukemia effect. Vox Sanguinis. 1998;74(Suppl. 2):341–343. - PubMed
-
- Briones J. Urbano-Ispizua A. Lawler M., et al. High frequency of donor chimerism after allogeneic transplantation of CD34+-selected peripheral blood cells. Exp. Hematol. 1998;26:415–420. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
