

Manometric features of eosinophilic esophagitis in esophageal pressure topography
- PMID: 21091849
- PMCID: PMC3036777
- DOI: 10.1111/j.1365-2982.2010.01633.x
Manometric features of eosinophilic esophagitis in esophageal pressure topography
Abstract
Background: Although most of the patients with eosinophilic esophagitis (EoE) have mucosal and structural changes that could potentially explain their symptoms, it is unclear whether EoE is associated with abnormal esophageal motor function. The aims of this study were to evaluate the esophageal pressure topography (EPT) findings in EoE and to compare them with controls and patients with gastro-esophageal disease (GERD).
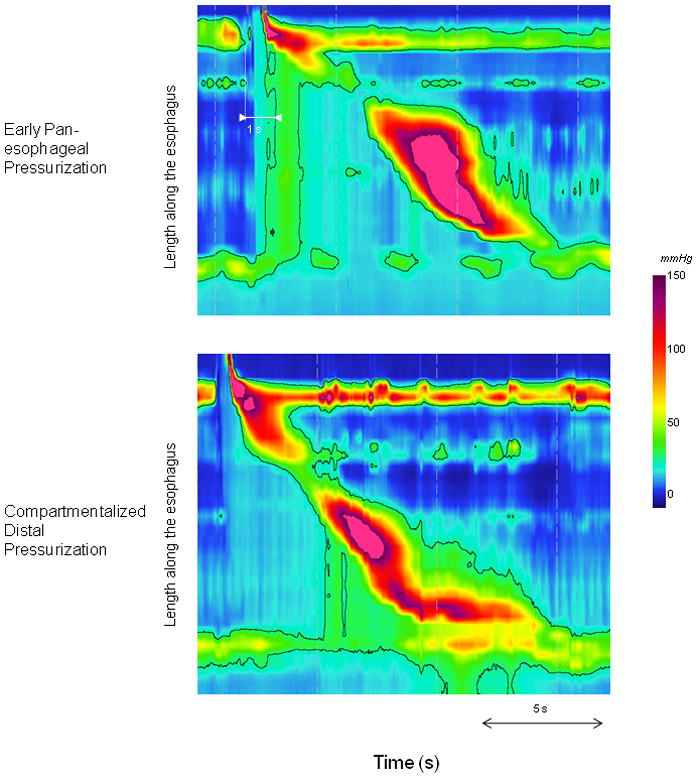
Methods: Esophageal pressure topography studies in 48 EoE patients, 48 GERD patients, and 50 controls were compared. The esophageal contractile pattern was described for ten 5-mL swallows for each subject and each swallow was secondarily characterized based on the bolus pressurization pattern: absent, pan-esophageal pressurization, or compartmentalized distal pressurization.
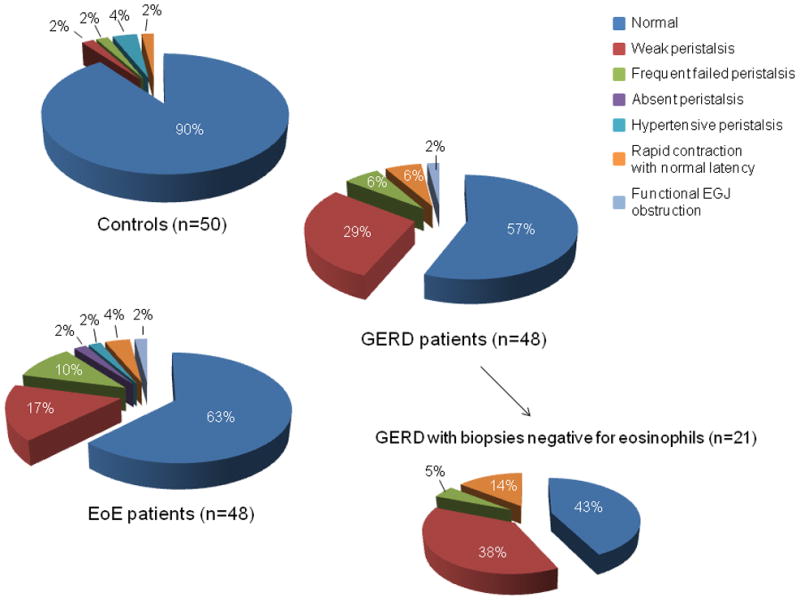
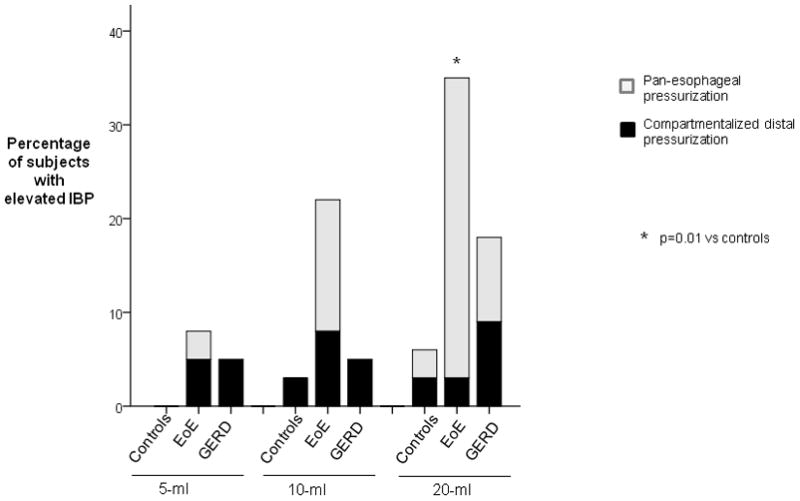
Key results: Thirty-seven percent of EoE patients were classified as having abnormal esophageal motility. The most frequent diagnoses were of weak peristalsis and frequent failed peristalsis. Although motility disorders were more frequent in EoE patients than in controls, the prevalence and type were similar to those observed in GERD patients (P=0.61, chi-square test). Pan-esophageal pressurization was present in 17% of EoE and 2% of GERD patients while compartmentalized pressurization was present in 19% of EoE and 10% of GERD patients. These patterns were not seen in control subjects.
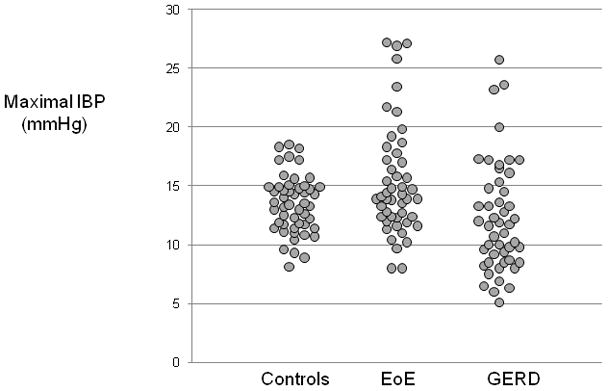
Conclusions & inferences: The prevalence of abnormal esophageal motility in EoE was approximately 37% and was similar in frequency and type to motor patterns observed in GERD. Eosinophilic esophagitis patients were more likely to have abnormal bolus pressurization patterns during swallowing and we hypothesize that this may be a manifestation of reduced esophageal compliance.
© 2010 Blackwell Publishing Ltd.
Conflict of interest statement
Figures
Similar articles
-
Esophageal motor abnormalities in eosinophilic esophagitis identified by high-resolution manometry.J Gastroenterol Hepatol. 2011 Sep;26(9):1447-50. doi: 10.1111/j.1440-1746.2011.06770.x. J Gastroenterol Hepatol. 2011. PMID: 21575059
-
Prevalence of esophageal motility abnormalities increases with longer disease duration in adult patients with eosinophilic esophagitis.Neurogastroenterol Motil. 2014 Sep;26(9):1349-55. doi: 10.1111/nmo.12400. Epub 2014 Jul 14. Neurogastroenterol Motil. 2014. PMID: 25039642
-
Development and Validation of a Mucosal Impedance Contour Analysis System to Distinguish Esophageal Disorders.Gastroenterology. 2019 May;156(6):1617-1626.e1. doi: 10.1053/j.gastro.2019.01.253. Epub 2019 Jan 31. Gastroenterology. 2019. PMID: 30711626 Free PMC article.
-
Esophageal dysmotility in patients with eosinophilic esophagitis: pathogenesis, assessment tools, manometric characteristics, and clinical implications.Esophagus. 2023 Jan;20(1):29-38. doi: 10.1007/s10388-022-00964-z. Epub 2022 Oct 11. Esophagus. 2023. PMID: 36220921 Free PMC article. Review.
-
Esophageal motility in eosinophilic esophagitis.Rev Gastroenterol Mex. 2015 Jul-Sep;80(3):205-13. doi: 10.1016/j.rgmx.2015.05.005. Epub 2015 Aug 12. Rev Gastroenterol Mex. 2015. PMID: 26275635 Review. English, Spanish.
Cited by
-
Biomechanics of esophageal function in eosinophilic esophagitis.J Neurogastroenterol Motil. 2012 Oct;18(4):357-64. doi: 10.5056/jnm.2012.18.4.357. Epub 2012 Oct 9. J Neurogastroenterol Motil. 2012. PMID: 23105995 Free PMC article.
-
Diagnosis and treatment of eosinophilic esophagitis in clinical practice.Clin J Gastroenterol. 2017 Apr;10(2):87-102. doi: 10.1007/s12328-017-0725-4. Epub 2017 Feb 28. Clin J Gastroenterol. 2017. PMID: 28247277 Review.
-
Eosinophilic esophagitis: current understanding and evolving concepts.Asia Pac Allergy. 2017 Jan;7(1):3-9. doi: 10.5415/apallergy.2017.7.1.3. Epub 2017 Jan 26. Asia Pac Allergy. 2017. PMID: 28154800 Free PMC article. Review.
-
Esophagitis and its causes: Who is "guilty" when acid is found "not guilty"?World J Gastroenterol. 2017 May 7;23(17):3011-3016. doi: 10.3748/wjg.v23.i17.3011. World J Gastroenterol. 2017. PMID: 28533657 Free PMC article.
-
Eosinophilic esophagitis: Current concepts in diagnosis and management.Saudi J Gastroenterol. 2024 Jul 1;30(4):210-227. doi: 10.4103/sjg.sjg_50_24. Epub 2024 May 16. Saudi J Gastroenterol. 2024. PMID: 38752302 Free PMC article. Review.
References
-
- Furuta GT, Liacouras CA, Collins MH, et al. Eosinophilic esophagitis in children and adults: a systematic review and consensus recommendations for diagnosis and treatment. Gastroenterology. 2007;133:1342–1363. - PubMed
-
- Fox VL. Eosinophilic esophagitis: endoscopic findings. Gastrointest Endosc Clin N Am. 2008;18:45–57. viii. - PubMed
-
- Stevoff C, Rao S, Parsons W, Kahrilas PJ, Hirano I. EUS and histopathologic correlates in eosinophilic esophagitis. Gastrointest Endosc. 2001;54:373–377. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
