

Long-term overall survival and metastasis-free survival for men with prostate-specific antigen-recurrent prostate cancer after prostatectomy: analysis of the Center for Prostate Disease Research National Database
- PMID: 21091976
- PMCID: PMC3402027
- DOI: 10.1111/j.1464-410X.2010.09878.x
Long-term overall survival and metastasis-free survival for men with prostate-specific antigen-recurrent prostate cancer after prostatectomy: analysis of the Center for Prostate Disease Research National Database
Abstract
Objective: • To describe metastasis-free survival (MFS) and overall survival (OS) among men with prostate-specific antigen (PSA)-recurrent prostate cancer after radical prostatectomy who did not receive additional therapy until metastasis, using a multicentre database capturing a wide ethnic mix.
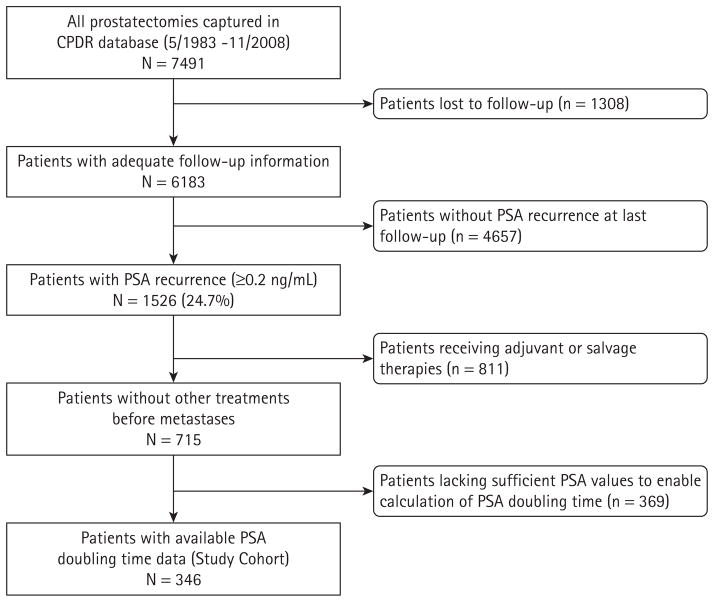
Patients and methods: • A retrospective analysis of the Center for Prostate Disease Research National Database (comprised of five US military hospitals and one civilian centre) was performed for patients with PSA relapse (≥ 0.2 ng/mL) after radical prostatectomy who had no additional therapy until the time of radiographic metastatic disease. • We investigated factors influencing metastasis and all-cause mortality using univariate and multivariate Cox regression analysis.
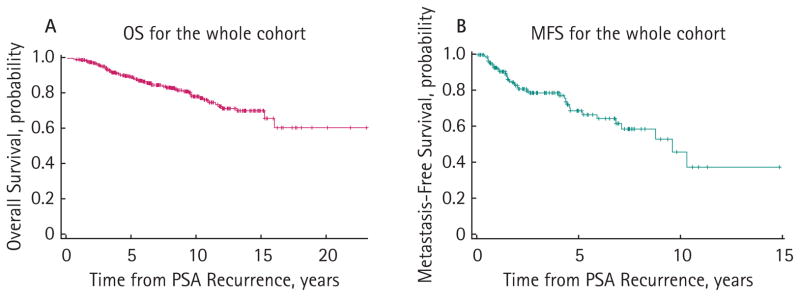
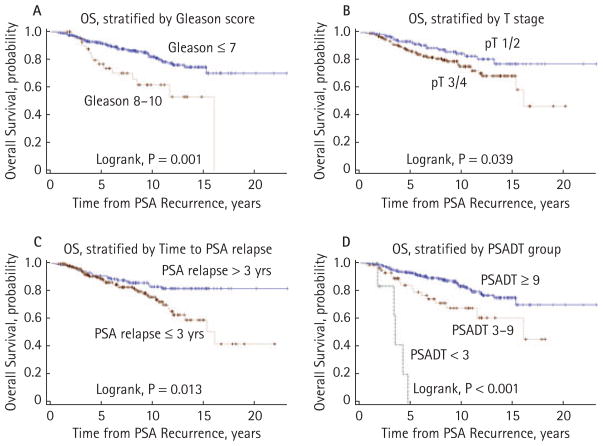
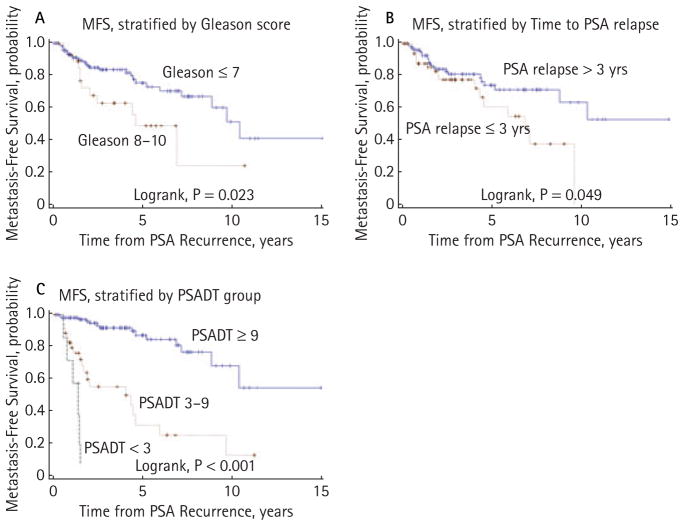
Results: • There were a total of 346 men who underwent radical prostatectomy between May 1983 and November 2008 and fulfilled the entry criteria. All patients had information on survival and 190 men had information on metastasis. Among patients with survival data (n= 346), 10-year OS was 79% after a median follow-up of 8.6 years from biochemical recurrence. • Among men with metastasis data (n= 190), 10-year MFS was 46% after a median follow-up of 7.5 years. • In Cox regressions, four clinical factors (Gleason score, pathological stage, time to PSA relapse and PSA doubling time), as well as age, were predictive of OS and/or MFS in univariate analysis, although only PSA doubling time (≥ 9 vs 3-8.9 vs <3 months) remained independently predictive of these outcomes in multivariate analysis (P < 0.001).
Conclusions: • This multicentre multi-ethnic dataset shows that OS and MFS can be extensive for men with PSA-recurrent prostate cancer, even in the absence of further therapy before metastasis. • This unique patient cohort, the second largest of its type after the Johns Hopkins cohort, confirms that PSA doubling time is the strongest determinant of OS and MFS in men with PSA-recurrent disease. • Longer follow-up and more events will be required to determine whether other variables may also contribute to these outcomes.
© 2010 THE AUTHORS. BJU INTERNATIONAL © 2010 BJU INTERNATIONAL.
Conflict of interest statement
None declared. Source of Funding: the present study was supported by the Department of Defense and the Congressional Special Interest (CSI) biomedical research programme.
Figures
References
-
- Jemal A, Siegel R, Xu J, Ward E. Cancer statistics, 2010. CA Cancer J Clin. 2010;60:277–300. - PubMed
-
- Roehl KA, Han M, Ramos CG, Antenor JA, Catalona WJ. Cancer progression and survival rates following anatomical radical retropubic prostatectomy in 3,478 consecutive patients: long-term results. J Urol. 2004;172:910–4. - PubMed
-
- Boccon-Gibod L, Djavan WB, Hammerer P, et al. Management of prostate-specific antigen relapse in prostate cancer: a European Consensus. Int J Clin Pract. 2004;58:382–90. - PubMed
-
- Sandler HM, Eisenberger MA. Assessing and treating patients with increasing prostate specific antigen following radical prostatectomy. J Urol. 2007;178:S20–4. - PubMed
-
- Messing EM, Manola J, Yao J, et al. Immediate versus deferred androgen deprivation treatment in patients with node-positive prostate cancer after radical prostatectomy and pelvic lymphadenectomy. Lancet Oncol. 2006;7:472–9. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
