

Validation of a new transpulmonary thermodilution system to assess global end-diastolic volume and extravascular lung water
- PMID: 21092252
- PMCID: PMC3220030
- DOI: 10.1186/cc9332
Validation of a new transpulmonary thermodilution system to assess global end-diastolic volume and extravascular lung water
Abstract
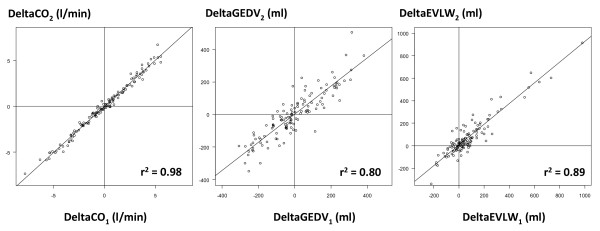
Introduction: A new system has been developed to assess global end-diastolic volume (GEDV), a volumetric marker of cardiac preload, and extravascular lung water (EVLW) from a transpulmonary thermodilution curve. Our goal was to compare this new system with the system currently in clinical use.
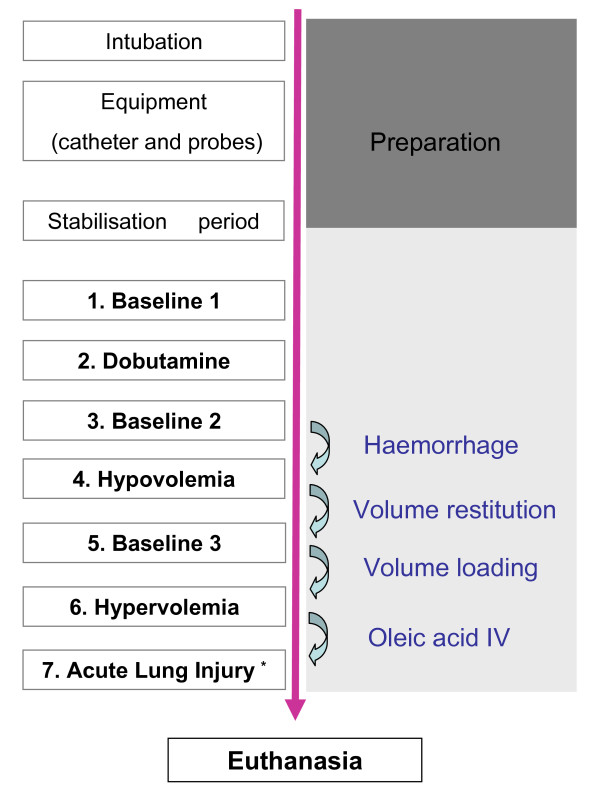
Methods: Eleven anesthetized and mechanically ventilated pigs were instrumented with a central venous catheter and a right (PulsioCath; Pulsion, Munich, Germany) and a left (VolumeView™; Edwards Lifesciences, Irvine, CA, USA) thermistor-tipped femoral arterial catheter. The right femoral catheter was used to measure GEDV and EVLW using the PiCCO(2)™ (Pulsion) method (GEDV(1) and EVLW(1), respectively). The left femoral catheter was used to measure the same parameters using the new VolumeView™ (Edwards Lifesciences) method (GEDV(2) and EVLW(2), respectively). Measurements were made during inotropic stimulation (dobutamine), during hypovolemia (bleeding), during hypervolemia (fluid overload), and after inducing acute lung injury (intravenous oleic acid).
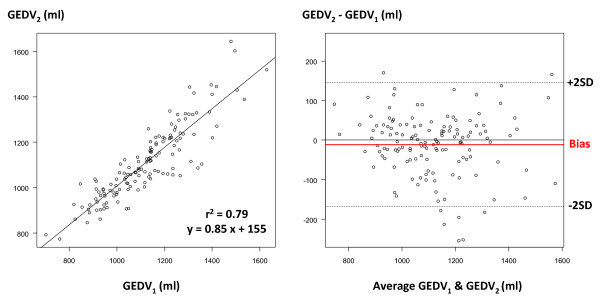
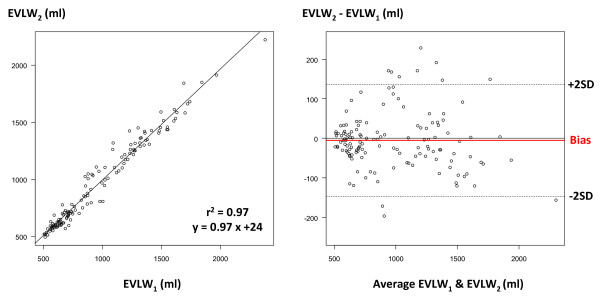
Results: One hundred and thirty-seven paired measurements were analyzed. GEDV(1) and GEDV(2) ranged from 701 to 1,629 ml and from 774 to 1,645 ml, respectively. GEDV(1) and GEDV(2) were closely correlated (r(2) = 0.79), with mean bias of -11 ± 80 ml and percentage error of 14%. EVLW(1) and EVLW(2) ranged from 507 to 2,379 ml and from 495 to 2,222 ml, respectively. EVLW(1) and EVLW(2) were closely correlated (r(2) = 0.97), with mean bias of -5 ± 72 ml and percentage error of 15%.
Conclusions: In animals, and over a very wide range of values, a good agreement was found between the new VolumeView™ system and the PiCCO™ system to assess GEDV and EVLW.
Figures

References
-
- Michard F, Perel A. In: Yearbook of Intensive Care and Emergency Medicine. Vincent JL, editor. Berlin: Springer; 2003. Management of circulatory and respiratory failure using less invasive hemodynamic monitoring; pp. 508–520.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
