

Delirium epidemiology in critical care (DECCA): an international study
- PMID: 21092264
- PMCID: PMC3220001
- DOI: 10.1186/cc9333
Delirium epidemiology in critical care (DECCA): an international study
Abstract
Introduction: Delirium is a frequent source of morbidity in intensive care units (ICUs). Most data on its epidemiology is from single-center studies. Our aim was to conduct a multicenter study to evaluate the epidemiology of delirium in the ICU.
Methods: A 1-day point-prevalence study was undertaken in 104 ICUs from 11 countries in South and North America and Spain.
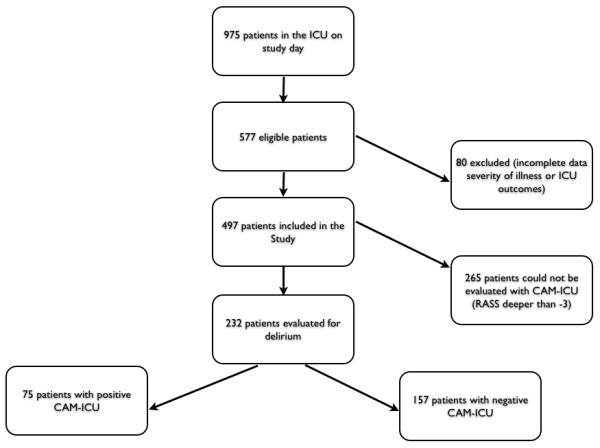
Results: In total, 975 patients were screened, and 497 fulfilled inclusion criteria and were enrolled (median age, 62 years; 52.5% men; 16.7% and 19.9% for ICU and hospital mortality); 64% were admitted to the ICU because of medical causes, and sepsis was the main diagnosis (n = 76; 15.3%). In total, 265 patients were sedated with the Richmond agitation and sedation scale (RASS) deeper than -3, and only 232 (46.6%) patients could be evaluated with the confusion-assessment method for the ICU. The prevalence of delirium was 32.3%. Compared with patients without delirium, those with the diagnosis of delirium had a greater severity of illness at admission, demonstrated by higher sequential organ-failure assessment (SOFA (P = 0.004)) and simplified acute physiology score 3 (SAPS3) scores (P < 0.0001). Delirium was associated with increased ICU (20% versus 5.7%; P = 0.002) and hospital mortality (24 versus 8.3%; P = 0.0017), and longer ICU (P < 0.0001) and hospital length of stay (LOS) (22 (11 to 40) versus 7 (4 to 18) days; P < 0.0001). Previous use of midazolam (P = 0.009) was more frequent in patients with delirium. On multivariate analysis, delirium was independently associated with increased ICU mortality (OR = 3.14 (1.26 to 7.86); CI, 95%) and hospital mortality (OR = 2.5 (1.1 to 5.7); CI, 95%).
Conclusions: In this 1-day international study, delirium was frequent and associated with increased mortality and ICU LOS. The main modifiable risk factors associated with the diagnosis of delirium were the use of invasive devices and sedatives (midazolam).
Comment in
-
Delirium in the ICU: time to probe the hard questions.Crit Care. 2011;15(1):118. doi: 10.1186/cc9971. Epub 2011 Feb 4. Crit Care. 2011. PMID: 21371353 Free PMC article.
References
-
- Morandi A, Pandharipande P, Trabucchi M, Rozzini R, Mistraletti G, Trompeo AC, Gregoretti C, Gattinoni L, Ranieri MV, Brochard L, Annane D, Putensen C, Guenther U, Fuentes P, Tobar E, Anzueto AR, Esteban A, Skrobik Y, Salluh JI, Soares M, Granja C, Stubhaug A, de Rooij SE, Ely EW. Understanding international differences in terminology for delirium and other types of acute brain dysfunction in critically ill patients. Intensive Care Med. 2008;34:1907–1915. doi: 10.1007/s00134-008-1177-6. - DOI - PubMed
-
- Ely EW, Inouye SK, Bernard GR, Gordon S, Francis J, May L, Truman B, Speroff T, Gautam S, Margolin R, Hart RP, Dittus R. Delirium in mechanically ventilated patients: validity and reliability of the confusion assessment method for the intensive care unit (CAM-ICU) JAMA. 2001;286:2703–2710. doi: 10.1001/jama.286.21.2703. - DOI - PubMed
-
- Devlin JW, Fong JJ, Howard EP, Skrobik Y, McCoy N, Yasuda C, Marshall J. Assessment of delirium in the intensive care unit: nursing practices and perceptions. Am J Crit Care. 2008;17:555–565; quiz 566. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
