

Should patient setup in lung cancer be based on the primary tumor? An analysis of tumor coverage and normal tissue dose using repeated positron emission tomography/computed tomography imaging
- PMID: 21093173
- PMCID: PMC4693613
- DOI: 10.1016/j.ijrobp.2010.09.016
Should patient setup in lung cancer be based on the primary tumor? An analysis of tumor coverage and normal tissue dose using repeated positron emission tomography/computed tomography imaging
Abstract
Purpose: Evaluation of the dose distribution for lung cancer patients using a patient setup procedure based on the bony anatomy or the primary tumor.
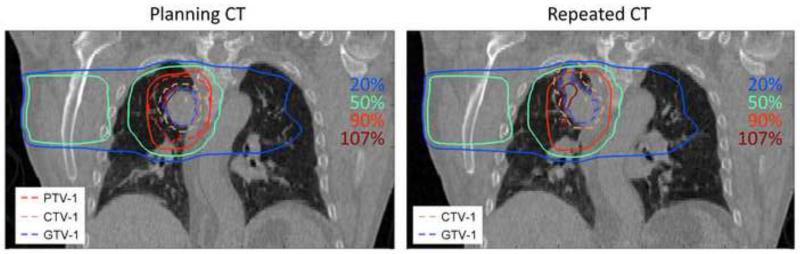
Methods and materials: For 39 patients with non-small-cell lung cancer, the planning fluorodeoxyglucose positron emission tomography/computed tomography (FDG-PET/CT) scan was registered to a repeated FDG-PET/CT scan made in the second week of treatment. Two patient setup methods were analyzed based on the bony anatomy or the primary tumor. The original treatment plan was copied to the repeated scan, and target and normal tissue structures were delineated. Dose distributions were analyzed using dose-volume histograms for the primary tumor, lymph nodes, lungs, and spinal cord.
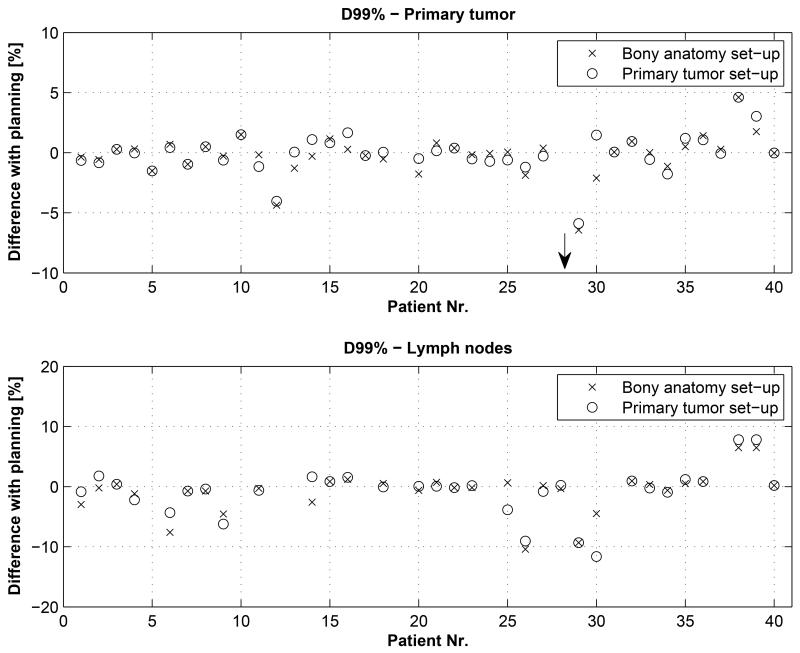
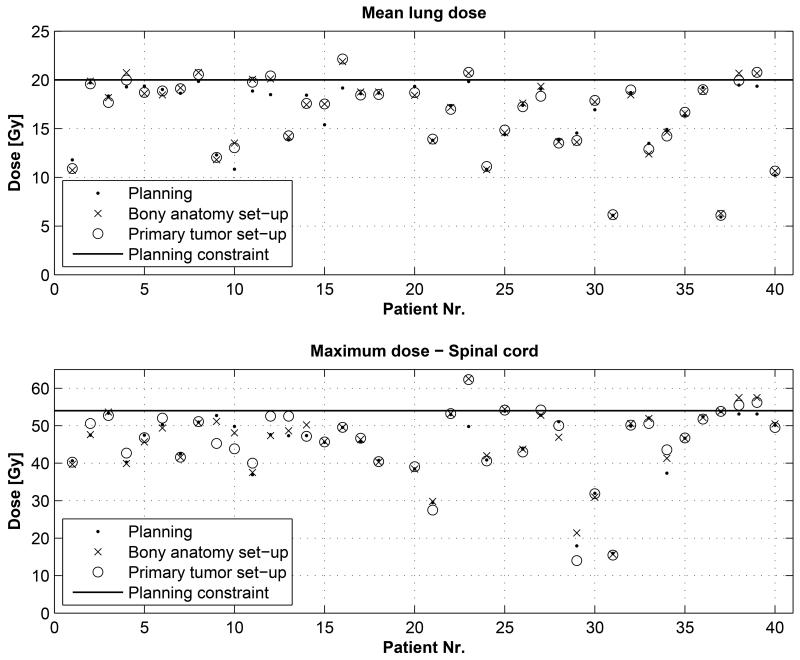
Results: One patient showed decreased dose coverage of the primary tumor caused by progressive disease and required replanning to achieve adequate coverage. For the other patients, the minimum dose to the primary tumor did not significantly deviate from the planned dose: -0.2 ± 1.7% (p = 0.71) and -0.1 ± 1.7% (p = 0.85) for the bony anatomy setup and the primary tumor setup, respectively. For patients (n = 31) with nodal involvement, 10% showed a decrease in minimum dose larger than 5% for the bony anatomy setup and 13% for the primary tumor setup. The mean lung dose exceeded the maximum allowed 20 Gy in 21% of the patients for the bony anatomy setup and in 13% for the primary tumor setup, whereas for the spinal cord this occurred in 10% and 13% of the patients, respectively.
Conclusions: In 10% and 13% of patients with nodal involvement, setup based on bony anatomy or primary tumor, respectively, led to important dose deviations in nodal target volumes. Overdosage of critical structures occurred in 10-20% of the patients. In cases of progressive disease, repeated imaging revealed underdosage of the primary tumor. Development of practical ways for setup procedures based on repeated high-quality imaging of all tumor sites during radiotherapy should therefore be an important research focus.
Copyright © 2012 Elsevier Inc. All rights reserved.
Figures
References
-
- Belderbos JS, Heemsbergen WD, De Jaeger K, et al. Final results of a Phase I/II dose escalation trial in non-small-cell lung cancer using three-dimensional conformal radiotherapy. Int J Radiat Oncol Biol Phys. 2006;66:126–134. - PubMed
-
- van Baardwijk A, Wanders S, Boersma L, et al. Mature results of an individualized radiation dose prescription study based on normal tissue constraints in stages I to III non-small-cell lung cancer. J Clin Oncol. 2010;28:1380–1386. - PubMed
-
- De Ruysscher D, Wanders S, van Haren E, et al. Selective mediastinal node irradiation based on FDG-PET scan data in patients with non-small-cell lung cancer: a prospective clinical study. Int J Radiat Oncol Biol Phys. 2005;62:988–994. - PubMed
-
- Bosmans G, van Baardwijk A, Dekker A, et al. Intra-patient variability of tumor volume and tumor motion during conventionally fractionated radiotherapy for locally advanced non-small-cell lung cancer: a prospective clinical study. Int J Radiat Oncol Biol Phys. 2006;66:748–753. - PubMed
-
- Fox J, Ford E, Redmond K, et al. Quantification of tumor volume changes during radiotherapy for non-small-cell lung cancer. Int J Radiat Oncol Biol Phys. 2009;74:341–348. - PubMed
