

A new electrocardiogram marker to identify patients at low risk for ventricular tachyarrhythmias: sum magnitude of the absolute QRST integral
- PMID: 21093871
- PMCID: PMC3058724
- DOI: 10.1016/j.jelectrocard.2010.08.012
A new electrocardiogram marker to identify patients at low risk for ventricular tachyarrhythmias: sum magnitude of the absolute QRST integral
Abstract
Objective: We proposed and tested a novel electrocardiogram marker of risk of ventricular arrhythmias (VAs).
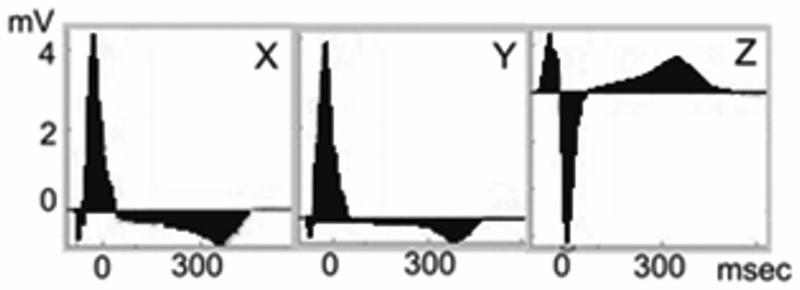
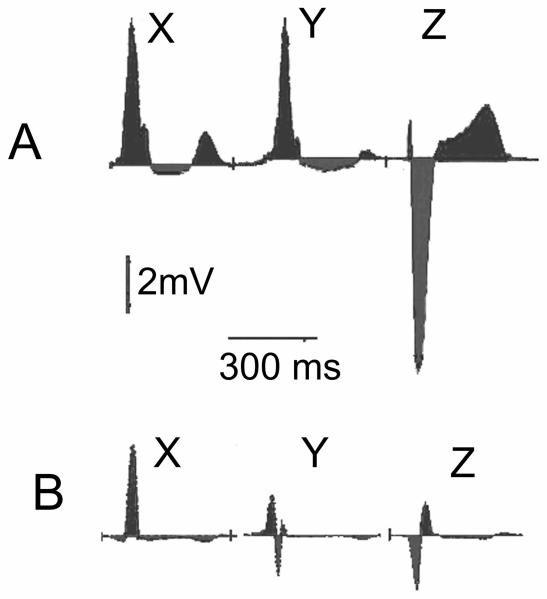
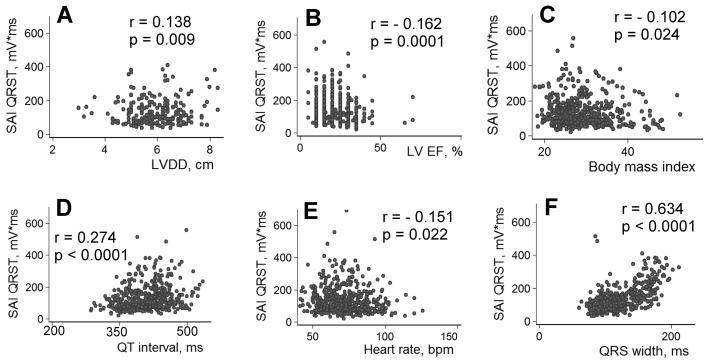
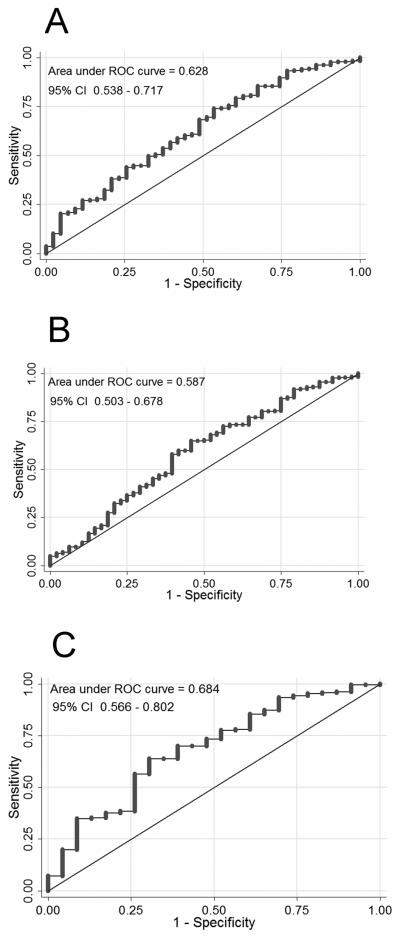
Methods: Digital orthogonal electrocardiograms were recorded at rest before implantable cardioverter-defibrillator (ICD) implantation in 508 participants of a primary prevention ICDs prospective cohort study (mean ± SD age, 60 ± 12 years; 377 male [74%]). The sum magnitude of the absolute QRST integral in 3 orthogonal leads (SAI QRST) was calculated. A derivation cohort of 128 patients was used to define a cutoff; a validation cohort (n = 380) was used to test a predictive value.
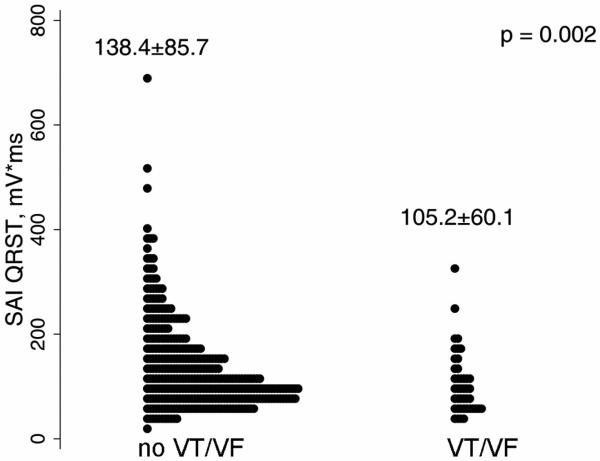
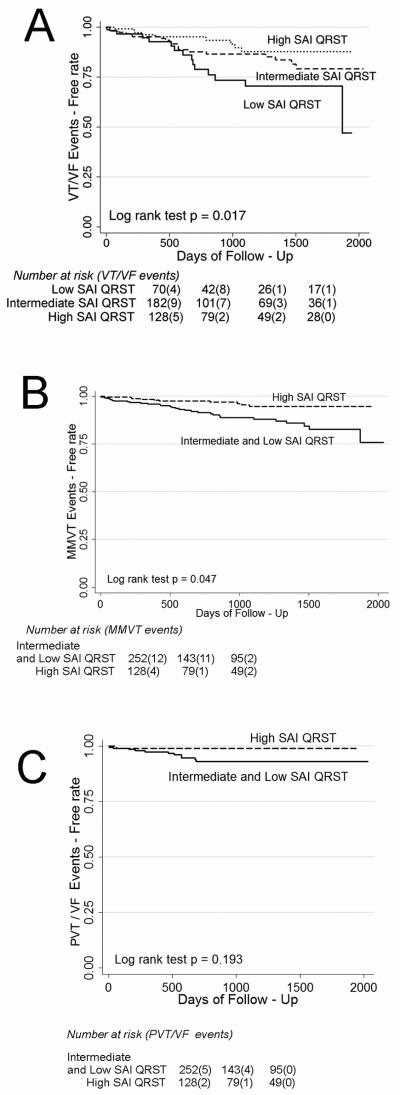
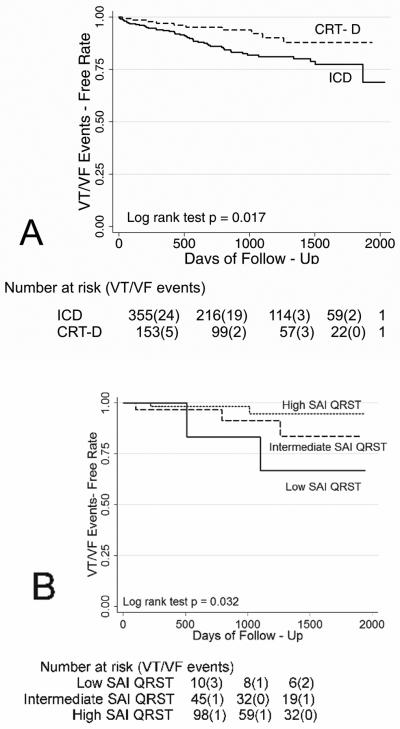
Results: During a mean follow-up of 18 months, 58 patients received appropriate ICD therapies. The SAI QRST was lower in patients with VA (105.2 ± 60.1 vs 138.4 ± 85.7 mV ms, P = .002). In the Cox proportional hazards analysis, patients with SAI QRST not exceeding 145 mV ms had about 4-fold higher risk of VA (hazard ratio, 3.6; 95% confidence interval, 1.96-6.71; P < .0001) and a 6-fold higher risk of monomorphic ventricular tachycardia (hazard ratio, 6.58; 95% confidence interval, 1.46-29.69; P = .014), whereas prediction of polymorphic ventricular tachycardia or ventricular fibrillation did not reach statistical significance.
Conclusion: High SAI QRST is associated with low risk of sustained VA in patients with structural heart disease.
Trial registration: ClinicalTrials.gov NCT00733590.
Copyright © 2011 Elsevier Inc. All rights reserved.
Figures
References
-
- Lloyd-Jones D, Adams R, Carnethon M, De SG, Ferguson TB, Flegal K, Ford E, Furie K, Go A, Greenlund K, Haase N, Hailpern S, Ho M, Howard V, Kissela B, Kittner S, Lackland D, Lisabeth L, Marelli A, McDermott M, Meigs J, Mozaffarian D, Nichol G, O'Donnell C, Roger V, Rosamond W, Sacco R, Sorlie P, Stafford R, Steinberger J, Thom T, Wasserthiel-Smoller S, Wong N, Wylie-Rosett J, Hong Y. Heart disease and stroke statistics--2009 update: a report from the American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Circulation. 2009;119:480–6. - PubMed
-
- A comparison of antiarrhythmic-drug therapy with implantable defibrillators in patients resuscitated from near-fatal ventricular arrhythmias. The Antiarrhythmics versus Implantable Defibrillators (AVID) Investigators. N Engl J Med. 1997;337:1576–83. - PubMed
-
- Moss AJ, Zareba W, Hall WJ, Klein H, Wilber DJ, Cannom DS, Daubert JP, Higgins SL, Brown MW, Andrews ML. Prophylactic implantation of a defibrillator in patients with myocardial infarction and reduced ejection fraction. N Engl J Med. 2002;346:877–83. - PubMed
-
- Bardy GH, Lee KL, Mark DB, Poole JE, Packer DL, Boineau R, Domanski M, Troutman C, Anderson J, Johnson G, McNulty SE, Clapp-Channing N, Davidson-Ray LD, Fraulo ES, Fishbein DP, Luceri RM, Ip JH. Amiodarone or an implantable cardioverter-defibrillator for congestive heart failure. N Engl J Med. 2005;352:225–37. - PubMed
-
- Goldenberg I, Vyas AK, Hall WJ, Moss AJ, Wang H, He H, Zareba W, McNitt S, Andrews ML. Risk stratification for primary implantation of a cardioverter-defibrillator in patients with ischemic left ventricular dysfunction. J Am Coll Cardiol. 2008;51:288–96. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
