

Survival of elderly patients with stage 5 CKD: comparison of conservative management and renal replacement therapy
- PMID: 21098012
- PMCID: PMC3084441
- DOI: 10.1093/ndt/gfq630
Survival of elderly patients with stage 5 CKD: comparison of conservative management and renal replacement therapy
Abstract
Background: Elderly patients with end-stage renal disease and severe extra-renal comorbidity have a poor prognosis on renal replacement therapy (RRT) and may opt to be managed conservatively (CM). Information on the survival of patients on this mode of therapy is limited.
Methods: We studied survival in a large cohort of CM patients in comparison to patients who received RRT.
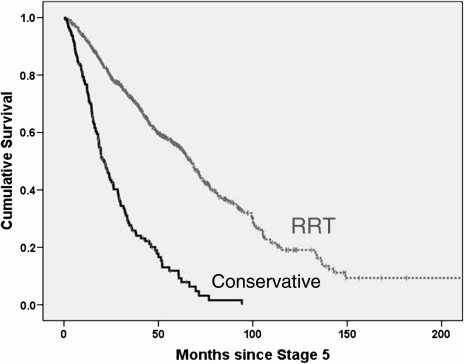
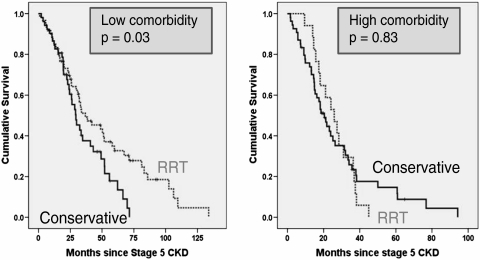
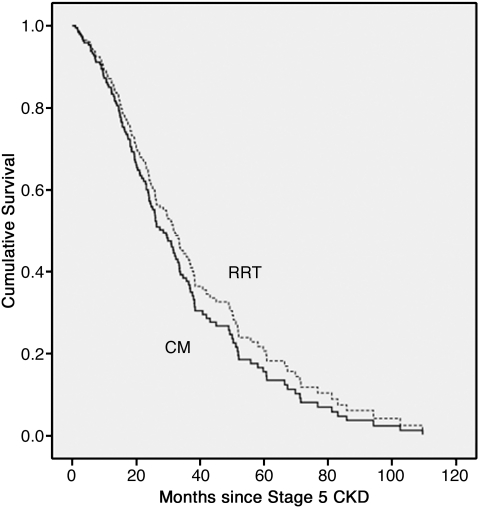
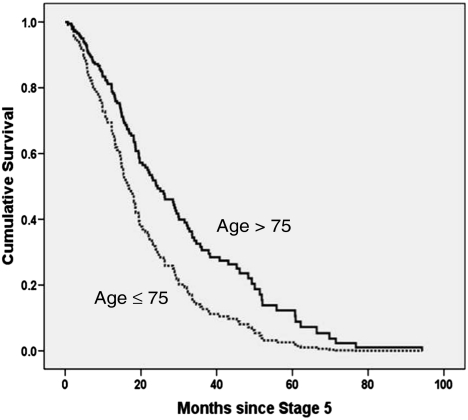
Results: Over an 18-year period, we studied 844 patients, 689 (82%) of whom had been treated by RRT and 155 (18%) were CM. CM patients were older and a greater proportion had high comorbidity. Median survival from entry into stage 5 chronic kidney disease was less in CM than in RRT (21.2 vs 67.1 months: P < 0.001). However, in patients aged > 75 years when corrected for age, high comorbidity and diabetes, the survival advantage from RRT was ~ 4 months, which was not statistically significant. Increasing age, the presence of high comorbidity and the presence of diabetes were independent determinants of poorer survival in RRT patients. In CM patients, however, age > 75 years and female gender independently predicted better survival.
Conclusions: In patients aged > 75 years with high extra-renal comorbidity, the survival advantage conferred by RRT over CM is likely to be small. Age > 75 years and female gender predicted better survival in CM patients. The reasons for this are unclear.
Figures
References
-
- Farrington K, Udayaraj U, Gilg J, et al. UK Renal Registry 11th Annual Report (December 2008): Chapter 3 ESRD incident rates in 2007 in the UK: national and centre-specific analyses. Nephron Clin Pract. 2009;111:c13–c41. - PubMed
-
- Zoccali C, Kramer A, Jager K. The databases: renal replacement therapy since 1989—the European Renal Association and European Dialysis and Transplant Association (ERA–EDTA) Clin J Am Soc Nephrol. 2009;4:S18–S22. - PubMed
-
- U S Renal Data System. USRDS 2009 Annual Data Report: Atlas of Chronic Kidney Disease and End-Stage Renal Disease in the United States. Bethesda, MD: National Institute of Diabetes and Digestive and Kidney Diseases; 2009.
