

Risk factors in children hospitalized with RSV bronchiolitis versus non-RSV bronchiolitis
- PMID: 21098154
- PMCID: PMC3761792
- DOI: 10.1542/peds.2010-0507
Risk factors in children hospitalized with RSV bronchiolitis versus non-RSV bronchiolitis
Abstract
Background: The trends in hospitalization rates and risk factors for severe bronchiolitis have not been recently described, especially after the routine implementation of prophylaxis for respiratory syncytial virus (RSV) infections.
Objectives: To define the burden of hospitalizations related to RSV and non-RSV bronchiolitis in a tertiary-care children's hospital from 2002 to 2007 and to identify the risk factors associated with severe disease.
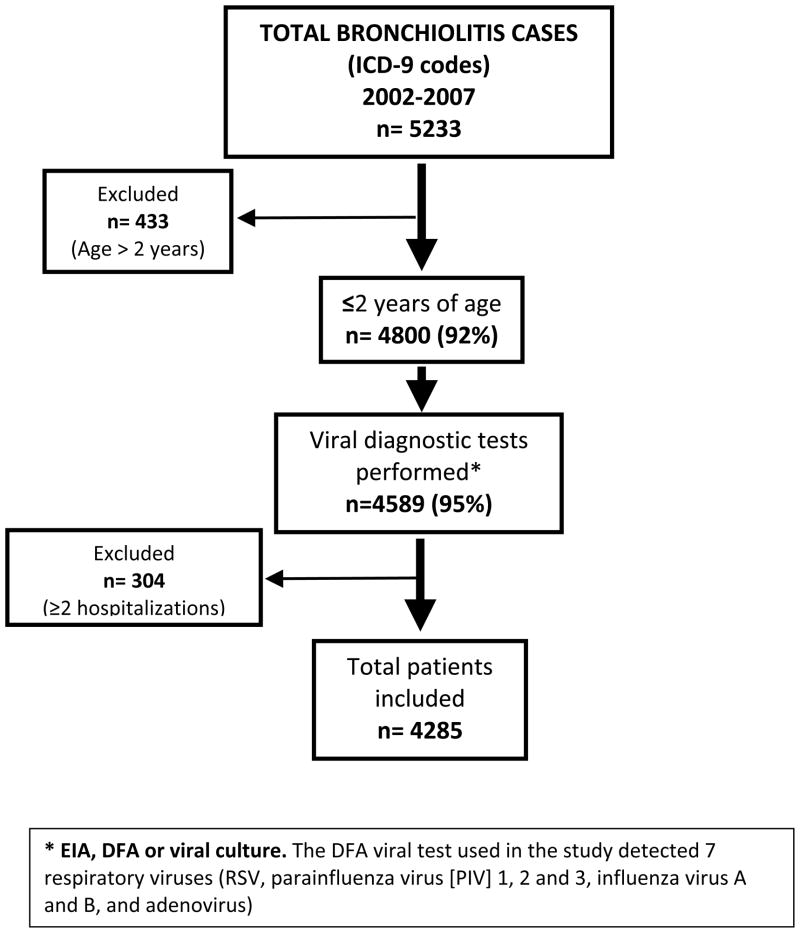
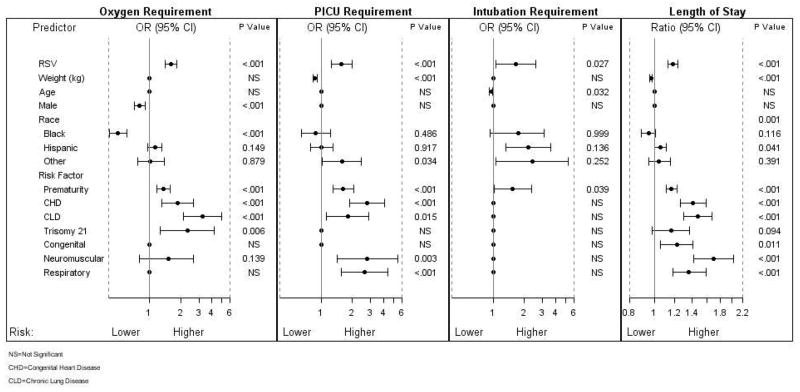
Methods: Medical records of patients hospitalized for bronchiolitis were reviewed for demographic, clinical, microbiologic, and radiologic characteristics as well as the presence of underlying medical conditions. Differences were evaluated between children with RSV and non-RSV bronchiolitis, and multivariable logistic regression analyses were performed to identify independent risk factors for severe disease.
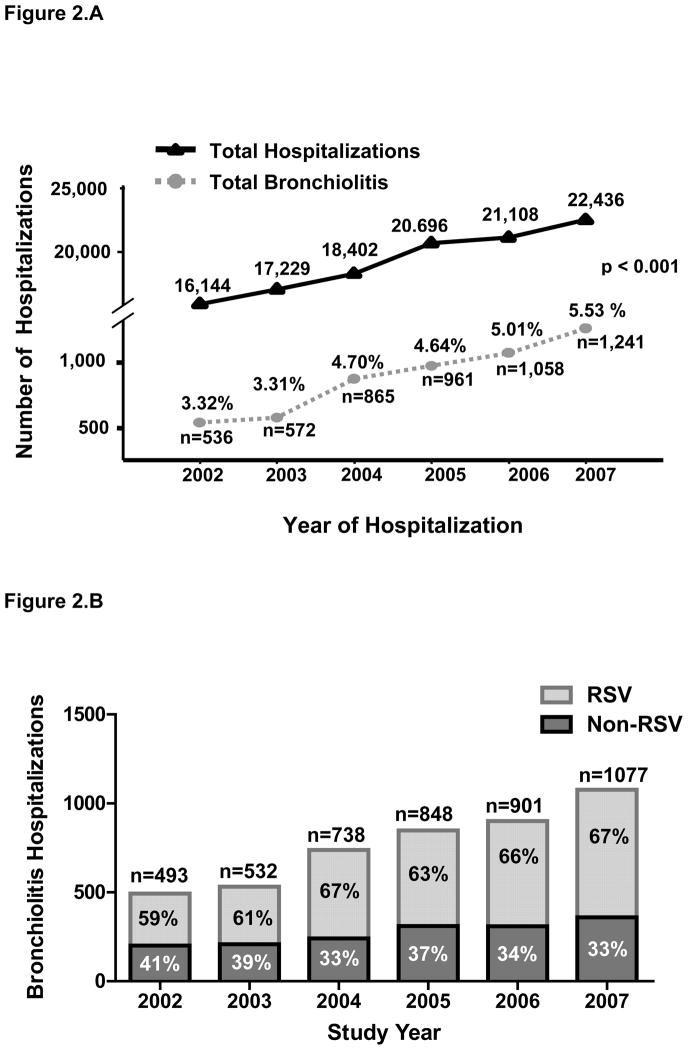
Results: Bronchiolitis hospitalizations in children younger than 2 years old (n = 4800) significantly increased from 536 (3.3%) in 2002 to 1241 (5.5%) in 2007, mainly because of RSV infections. Patients with RSV bronchiolitis (n = 2840 [66%]) were younger at hospitalization and had a lower percentage of underlying medical conditions than children hospitalized with non-RSV bronchiolitis (27 vs 37.5%; P < .001). However, disease severity defined by length of hospitalization and requirement of supplemental oxygen, intensive care, and mechanical ventilation was significantly worse in children with RSV bronchiolitis. RSV infection and prematurity, regardless of the etiology, were identified as independent risk factors for severe bronchiolitis.
Conclusions: There was a significant increase in hospitalizations for RSV bronchiolitis from 2002 to 2007. A majority of the children with RSV bronchiolitis were previously healthy, but their disease severity was worse compared with those hospitalized with non-RSV bronchiolitis.
Figures
References
-
- Shay DK, Holman RC, Newman RD, Liu LL, Stout JW, Anderson LJ. Bronchiolitis-associated hospitalizations among US children, 1980–1996. JAMA. 1999;282(15):1440–1446. - PubMed
-
- Boyce TG, Mellen BG, Mitchel EF, Jr, Wright PF, Griffin MR. Rates of hospitalization for respiratory syncytial virus infection among children in Medicaid. J Pediatr. 2000;137(6):865–870. - PubMed
-
- Leader S, Kohlhase K. Respiratory syncytial virus-coded pediatric hospitalizations, 1997 to 1999. Pediatr Infect Dis J. 2002;21(7):629–632. - PubMed
-
- Leader S, Kohlhase K. Recent trends in severe respiratory syncytial virus (RSV) among US infants, 1997 to 2000. J Pediatr. 2003;143(5 suppl):S127–S132. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
