

In silico children and the glass mouse model: clinical trial simulations to identify and individualize optimal isoniazid doses in children with tuberculosis
- PMID: 21098246
- PMCID: PMC3028779
- DOI: 10.1128/AAC.00763-10
In silico children and the glass mouse model: clinical trial simulations to identify and individualize optimal isoniazid doses in children with tuberculosis
Abstract
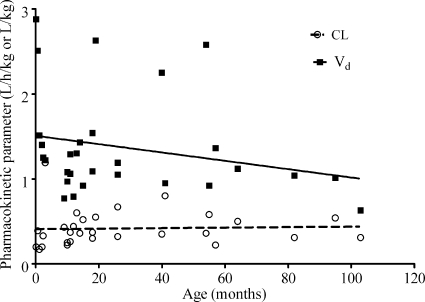
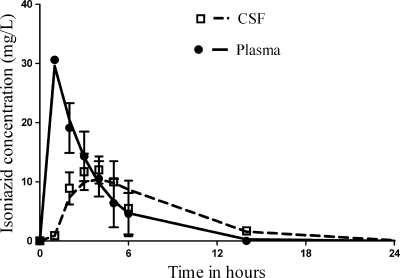
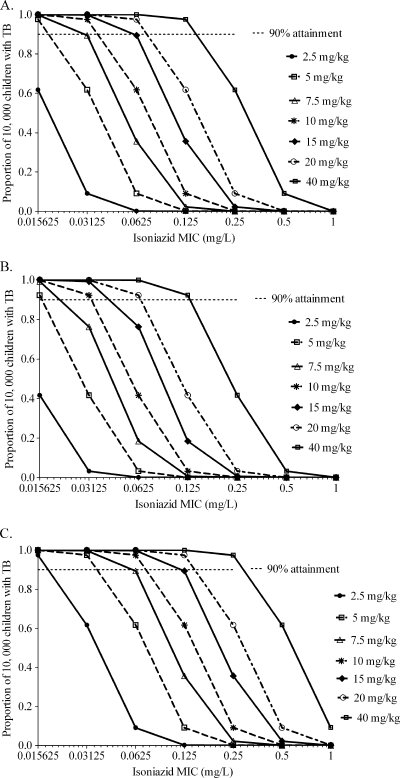
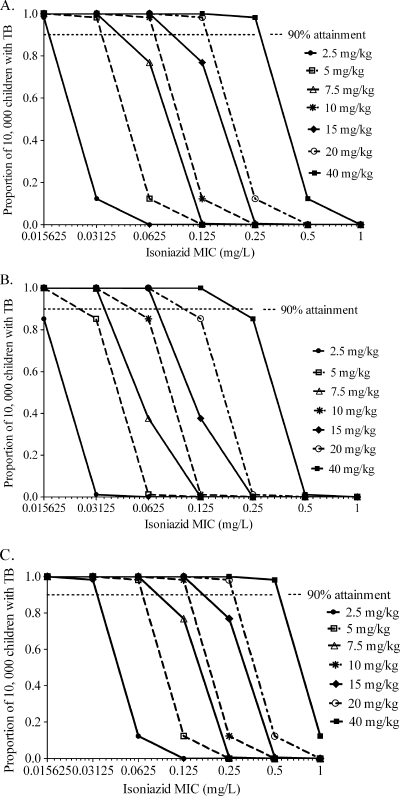
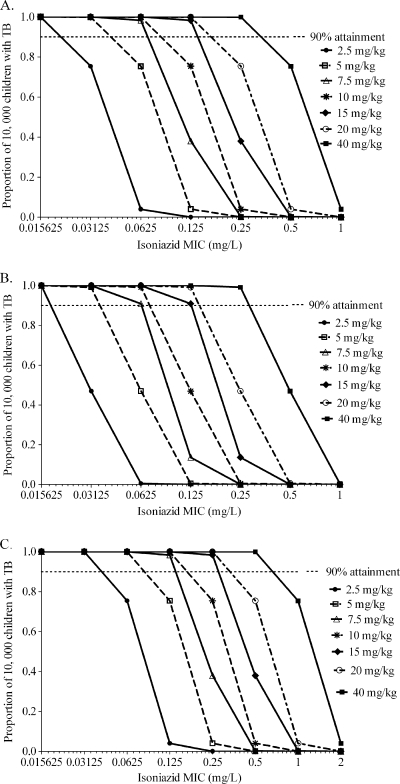
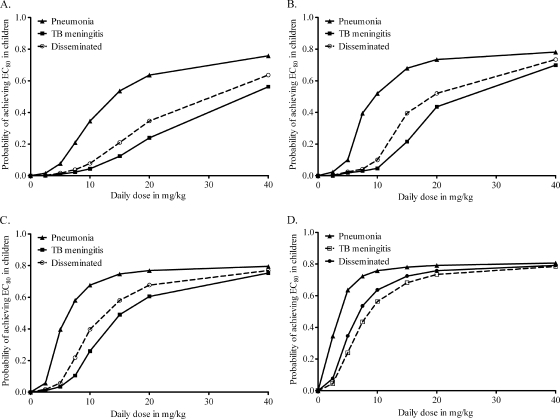
Children with tuberculosis present with high rates of disseminated disease and tuberculous (TB) meningitis due to poor cell-mediated immunity. Recommended isoniazid doses vary from 5 mg/kg/day to 15 mg/kg/day. Antimicrobial pharmacokinetic/pharmacodynamic studies have demonstrated that the ratio of the 0- to 24-h area under the concentration-time curve (AUC(0-24)) to the MIC best explains isoniazid microbial kill. The AUC(0-24)/MIC ratio associated with 80% of maximal kill (80% effective concentration [EC(80)]), considered the optimal effect, is 287.2. Given the pharmacokinetics of isoniazid encountered in children 10 years old or younger, with infants as a special group, and given the differences in penetration of isoniazid into phagocytic cells, epithelial lining fluid, and subarachnoid space during TB meningitis, we performed 10,000 patient Monte Carlo simulations to determine how well isoniazid doses of between 2.5 and 40 mg/kg/day would achieve or exceed the EC(80). None of the doses examined achieved the EC(80) in ≥90% of children. Doses of 5 mg/kg were universally inferior; doses of 10 to 15 mg/kg/day were adequate only under the very limited circumstances of children who were slow acetylators and had disease limited to pneumonia. Each of the three disease syndromes, acetylation phenotype, and being an infant required different doses to achieve adequate AUC(0-24)/MIC exposures in an acceptable proportion of children. We conclude that current recommended doses for children are likely suboptimal and that isoniazid doses in children are best individualized based on disease process, age, and acetylation status.
Figures
References
-
- Ambrose, P. G., et al. 2007. Pharmacokinetics-pharmacodynamics of antimicrobial therapy: it's not just for mice anymore. Clin. Infect. Dis. 44:79-86. - PubMed
-
- Blumberg, H. M., et al. 2003. American Thoracic Society/Centers for Disease Control and Prevention/Infectious Diseases Society of America: treatment of tuberculosis. Am. J. Respir. Crit. Care Med. 167:603-662. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
