

Phase III, randomized study of the effects of parenteral iron, oral iron, or no iron supplementation on the erythropoietic response to darbepoetin alfa for patients with chemotherapy-associated anemia
- PMID: 21098317
- PMCID: PMC3055863
- DOI: 10.1200/JCO.2010.30.3644
Phase III, randomized study of the effects of parenteral iron, oral iron, or no iron supplementation on the erythropoietic response to darbepoetin alfa for patients with chemotherapy-associated anemia
Abstract
Purpose: Functional iron deficiency may impair response to erythropoiesis-stimulating agents (ESAs) in iron-replete patients with chemotherapy-associated anemia (CAA). This study evaluated whether coadministration of parenteral iron improves ESA efficacy in patients with CAA.
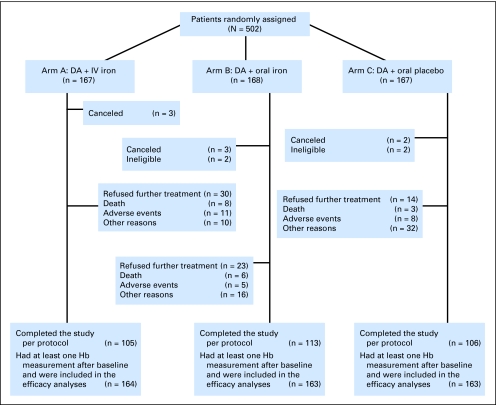
Patients and methods: This prospective, multicenter, randomized trial enrolled 502 patients with hemoglobin (Hb) less than 11 g/dL who were undergoing chemotherapy for nonmyeloid malignancies. All patients received darbepoetin alfa once every 3 weeks and were randomly assigned to receive either ferric gluconate 187.5 mg intravenously (IV) every 3 weeks, oral daily ferrous sulfate 325 mg, or oral placebo for 16 weeks.
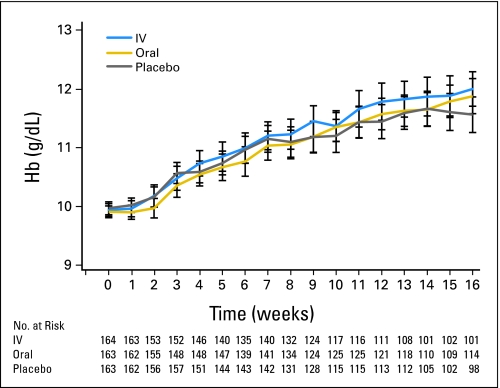
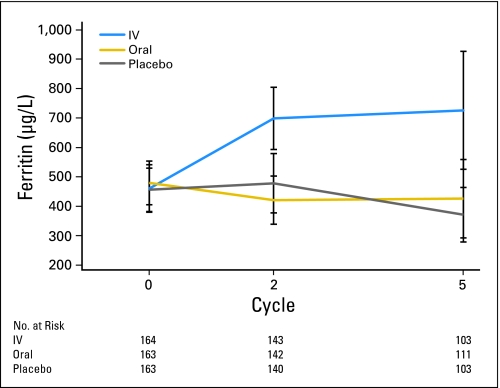
Results: There was no difference in the erythropoietic response rate (ie, proportion of patients achieving Hb ≥ 12 g/dL or Hb increase ≥ 2 g/dL from baseline): 69.5% (95% CI, 61.9% to 76.5%) of IV iron-treated patients achieved an erythropoietic response compared with 66.9% (95% CI, 59.1% to 74.0%) who received oral iron and 65.0% (95% CI, 57.2% to 72.3%) who received oral placebo (P = .75). There were also no differences in the proportion of patients requiring red cell transfusions, changes in quality of life, or the dose of darbepoetin administered. Adverse events (AEs) tended to be more common in the IV iron arm: grade 3 or higher AEs occurred in 54% (95% CI, 46% to 61%) of patients receiving IV iron compared with 44% (95% CI, 36% to 52%) who received oral iron and 46% (95% CI, 38% to 54%) who received oral placebo (P = .16).
Conclusion: In patients with CAA, addition of IV ferric gluconate to darbepoetin failed to provide additional benefit compared with oral iron or oral placebo.
Conflict of interest statement
Authors' disclosures of potential conflicts of interest and author contributions are found at the end of this article.
Figures
Comment in
-
Too-low iron doses and too many dropouts in negative iron trial?J Clin Oncol. 2011 Jun 10;29(17):e525-6; author reply e527-8. doi: 10.1200/JCO.2011.35.3219. Epub 2011 May 2. J Clin Oncol. 2011. PMID: 21537041 No abstract available.
References
-
- Spivak JL. The anaemia of cancer: Death by a thousand cuts. Nat Rev Cancer. 2005;5:543–555. - PubMed
-
- Bohlius J, Wilson J, Seidenfeld J, et al. Erythropoietin or darbepoetin for patients with cancer. Cochrane Database Syst Rev. 2006;3:CD003407. - PubMed
-
- Goodnough LT. Erythropoietin and iron-restricted erythropoiesis. Exp Hematol. 2007;35:167–172. - PubMed
-
- Bohlius J. Is intravenous iron supplementation with erythropoiesis-stimulating agents beneficial in cancer patients with anemia? Nat Clin Pract Oncol. 2008;5:688–689. - PubMed
-
- Auerbach M. Should intravenous iron be the standard of care in oncology? J Clin Oncol. 2008;26:1579–1581. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
