

Validation of an atrial fibrillation risk algorithm in whites and African Americans
- PMID: 21098350
- PMCID: PMC3021784
- DOI: 10.1001/archinternmed.2010.434
Validation of an atrial fibrillation risk algorithm in whites and African Americans
Abstract
Background: We sought to validate a recently published risk algorithm for incident atrial fibrillation (AF) in independent cohorts and other racial groups.
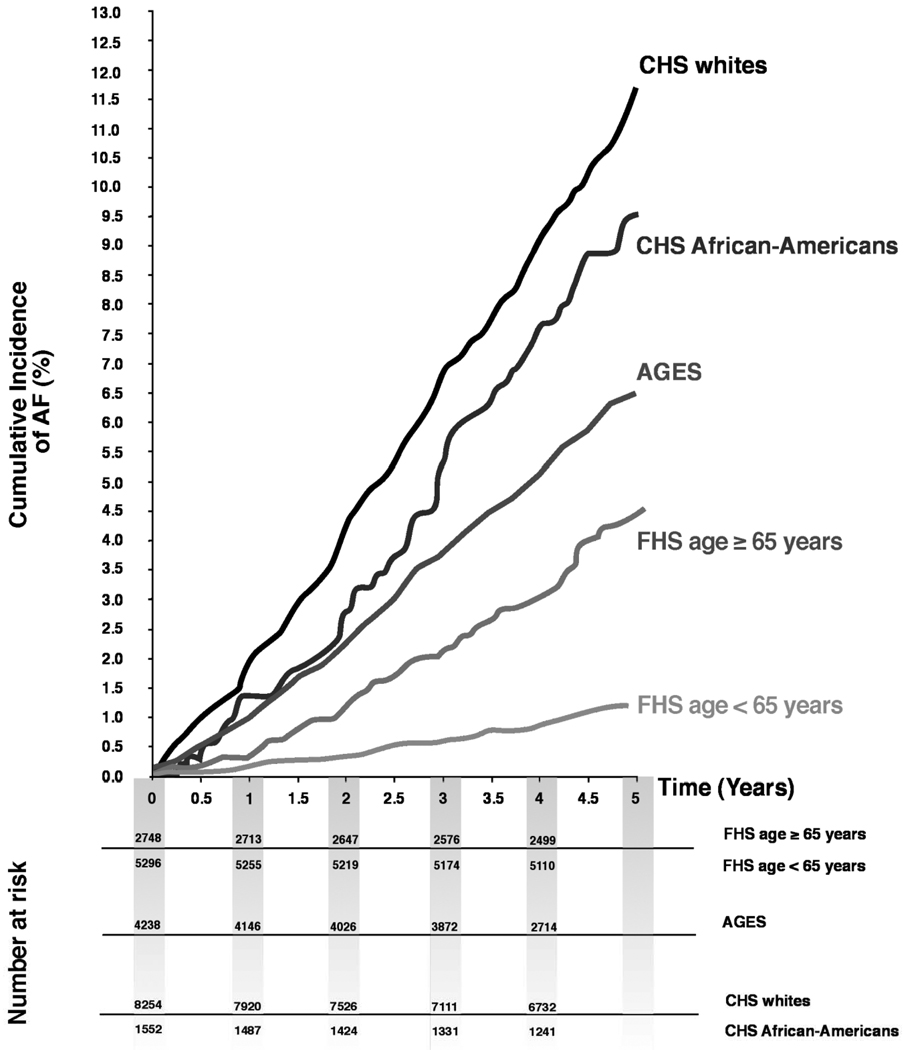
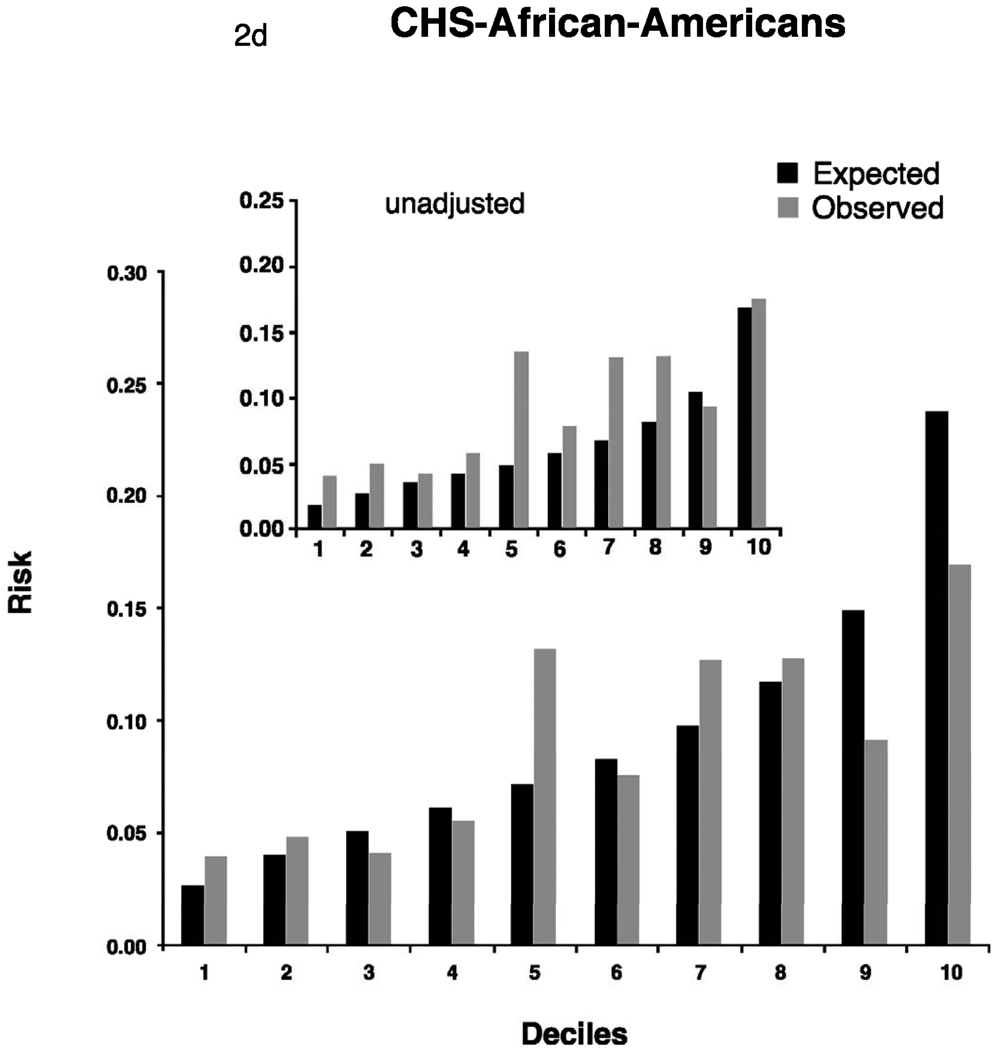
Methods: We evaluated the performance of a Framingham Heart Study (FHS)-derived risk algorithm modified for 5-year incidence of AF in the FHS (n = 4764 participants) and 2 geographically and racially diverse cohorts in the age range 45 to 95 years: AGES (the Age, Gene/Environment Susceptibility-Reykjavik Study) (n = 4238) and CHS (the Cardiovascular Health Study) (n = 5410, of whom 874 [16.2%] were African Americans). The risk algorithm included age, sex, body mass index, systolic blood pressure, electrocardiographic PR interval, hypertension treatment, and heart failure.
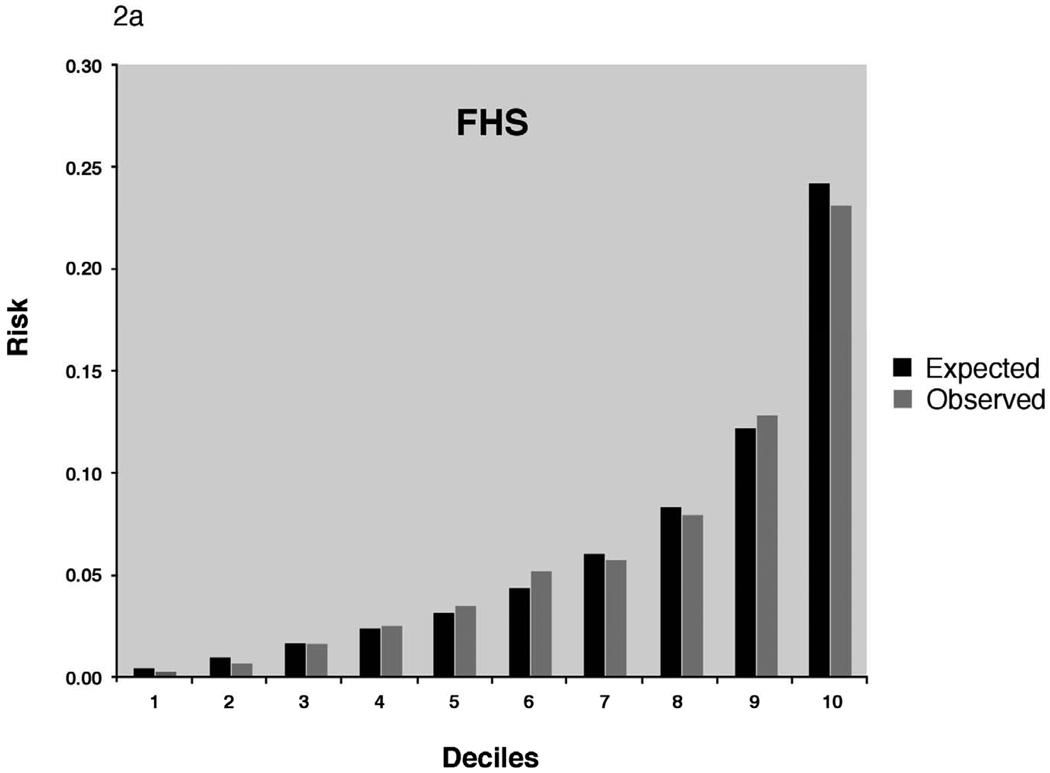
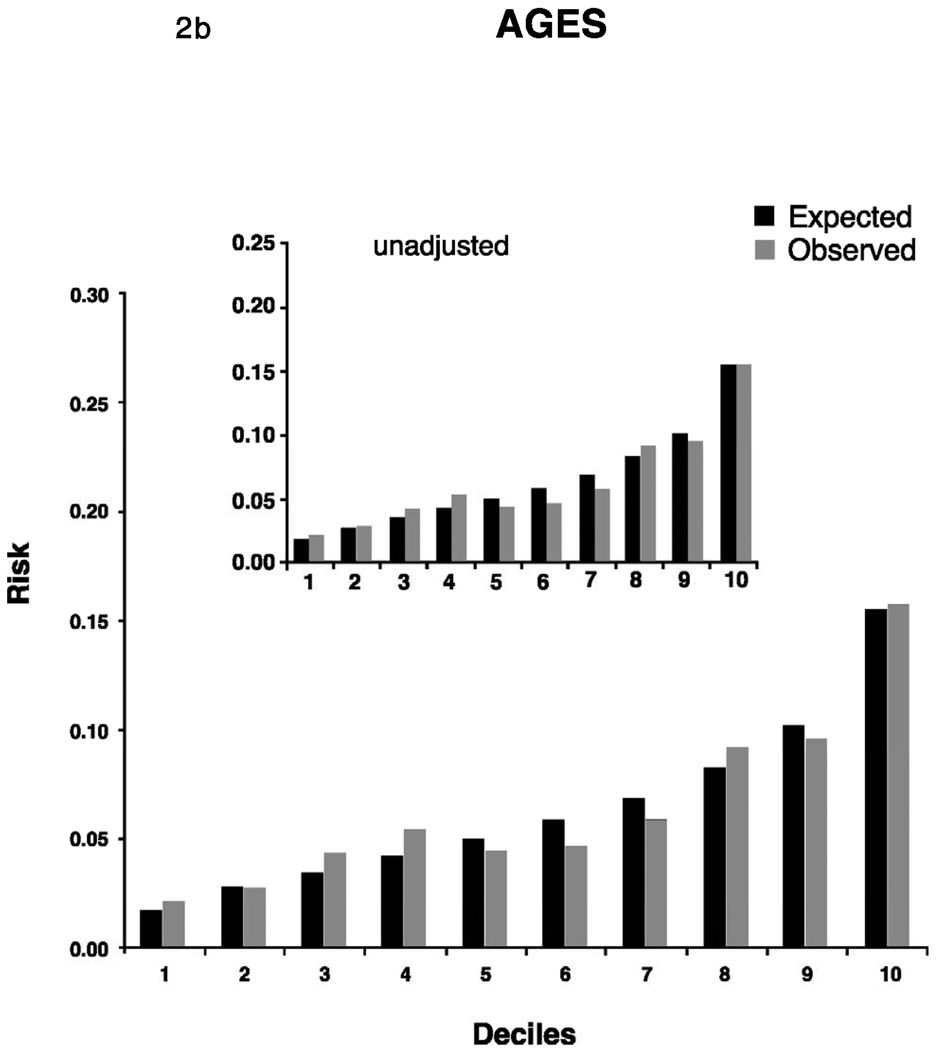
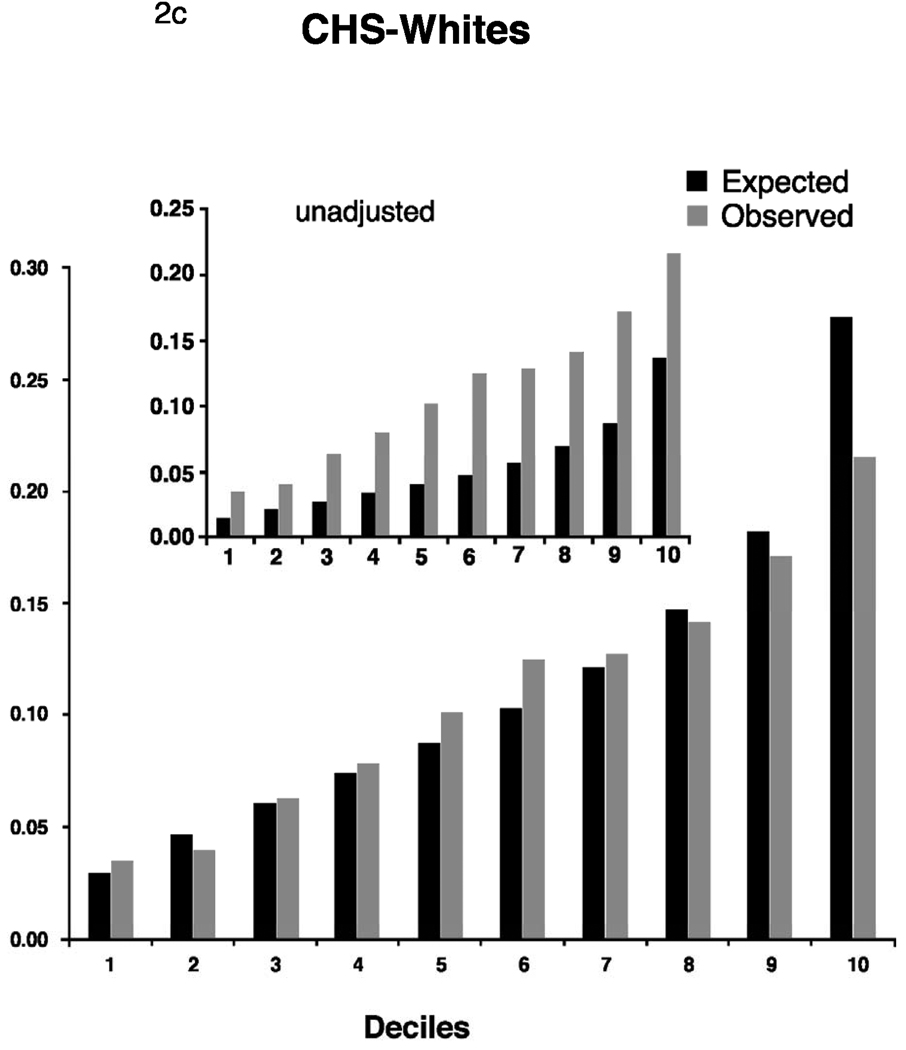
Results: We found 1359 incident AF events in 100 074 person-years of follow-up. Unadjusted 5-year event rates differed by cohort (AGES, 12.8 cases/1000 person-years; CHS whites, 22.7 cases/1000 person-years; and FHS, 4.5 cases/1000 person-years) and by race (CHS African Americans, 18.4 cases/1000 person-years). The strongest risk factors in all samples were age and heart failure. The relative risks for incident AF associated with risk factors were comparable across cohorts and race groups. After recalibration for baseline incidence and risk factor distribution, the Framingham algorithm, reported in C statistic, performed reasonably well in all samples: AGES, 0.67 (95% confidence interval [CI], 0.64-0.71); CHS whites, 0.68 (95% CI, 0.66-0.70); and CHS African Americans, 0.66 (95% CI, 0.61-0.71). Risk factors combined in the algorithm explained between 47.0% (AGES) and 63.6% (FHS) of the population-attributable risk.
Conclusions: Risk of incident AF in community-dwelling whites and African Americans can be assessed reliably by routinely available and potentially modifiable clinical variables. Seven risk factors accounted for up to 64% of risk.
Conflict of interest statement
There are no conflicts of interest to be reported by the authors.
Figures
Comment in
-
Predicting incident atrial fibrillation: an important step toward primary prevention.Arch Intern Med. 2010 Nov 22;170(21):1874-5. doi: 10.1001/archinternmed.2010.426. Arch Intern Med. 2010. PMID: 21098344 No abstract available.
-
Improving the prediction of incident atrial fibrillation.Arch Intern Med. 2011 Jun 27;171(12):1125; author reply 1125. doi: 10.1001/archinternmed.2011.266. Arch Intern Med. 2011. PMID: 21709121 No abstract available.
References
-
- Go AS, Hylek EM, Phillips KA, et al. Prevalence of diagnosed atrial fibrillation in adults: national implications for rhythm management and stroke prevention: the AnTicoagulation and Risk Factors in Atrial Fibrillation (ATRIA) Study. JAMA. 2001;285:2370–2375. - PubMed
-
- Miyasaka Y, Barnes ME, Gersh BJ, et al. Secular trends in incidence of atrial fibrillation in Olmsted County, Minnesota, 1980 to 2000, and implications on the projections for future prevalence. Circulation. 2006;114:119–125. - PubMed
-
- Borzecki AM, Bridgers DK, Liebschutz JM, Kader B, Kazis LE, Berlowitz DR. Racial differences in the prevalence of atrial fibrillation among males. J Natl Med Assoc. 2008;100:237–245. - PubMed
Publication types
MeSH terms
Grants and funding
- N01-HC-25195/HC/NHLBI NIH HHS/United States
- N01 HC085086/HC/NHLBI NIH HHS/United States
- N01 AG012100/AG/NIA NIH HHS/United States
- U01 HL080295/HL/NHLBI NIH HHS/United States
- N01 HC085085/HC/NHLBI NIH HHS/United States
- AG028321/AG/NIA NIH HHS/United States
- N01 HC025195/HL/NHLBI NIH HHS/United States
- N01 HC085079/HL/NHLBI NIH HHS/United States
- R01 HL080295/HL/NHLBI NIH HHS/United States
- N01 HC085084/HC/NHLBI NIH HHS/United States
- N01 HC-85084/HC/NHLBI NIH HHS/United States
- 2K24 HL04334/HL/NHLBI NIH HHS/United States
- N01 HC035129/HC/NHLBI NIH HHS/United States
- HL092577/HL/NHLBI NIH HHS/United States
- R01 NS017950/NS/NINDS NIH HHS/United States
- R01 NS 17950/NS/NINDS NIH HHS/United States
- N01 HC-85080/HC/NHLBI NIH HHS/United States
- N01 HC085081/HC/NHLBI NIH HHS/United States
- R01 HL092577/HL/NHLBI NIH HHS/United States
- R01 HL068986/HL/NHLBI NIH HHS/United States
- N01 HC-85082/HC/NHLBI NIH HHS/United States
- N01 HC015103/HC/NHLBI NIH HHS/United States
- N01 HC085086/HL/NHLBI NIH HHS/United States
- N01 HC085083/HC/NHLBI NIH HHS/United States
- N01 HC-85085/HC/NHLBI NIH HHS/United States
- N01 HC025195/HC/NHLBI NIH HHS/United States
- N01 HC-85081/HC/NHLBI NIH HHS/United States
- N01 HC-85079/HC/NHLBI NIH HHS/United States
- AG029451/AG/NIA NIH HHS/United States
- R01 HL087652/HL/NHLBI NIH HHS/United States
- RC1 HL101056/HL/NHLBI NIH HHS/United States
- R56 AG029451/AG/NIA NIH HHS/United States
- K24 HL004334/HL/NHLBI NIH HHS/United States
- N01 HC085082/HC/NHLBI NIH HHS/United States
- N01 HC-85086/HC/NHLBI NIH HHS/United States
- N01 HC085080/HC/NHLBI NIH HHS/United States
- N01 HC-55222/HC/NHLBI NIH HHS/United States
- N01 HC-85083/HC/NHLBI NIH HHS/United States
- N01 HC055222/HL/NHLBI NIH HHS/United States
- N01 HC055222/HC/NHLBI NIH HHS/United States
- R01 AG029451/AG/NIA NIH HHS/United States
- N01 HC085079/HC/NHLBI NIH HHS/United States
- R01 AG028321/AG/NIA NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
Research Materials
