

Plectin-1 as a novel biomarker for pancreatic cancer
- PMID: 21098698
- PMCID: PMC3044444
- DOI: 10.1158/1078-0432.CCR-10-0999
Plectin-1 as a novel biomarker for pancreatic cancer
Abstract
Purpose: We are in great need of specific biomarkers to detect pancreatic ductal adenocarcinoma (PDAC) at an early stage, ideally before invasion. Plectin-1 (Plec1) was recently identified as one such biomarker. However, its suitability as a specific biomarker for human pancreatic cancer, and its usability as an imaging target, remain to be assessed.
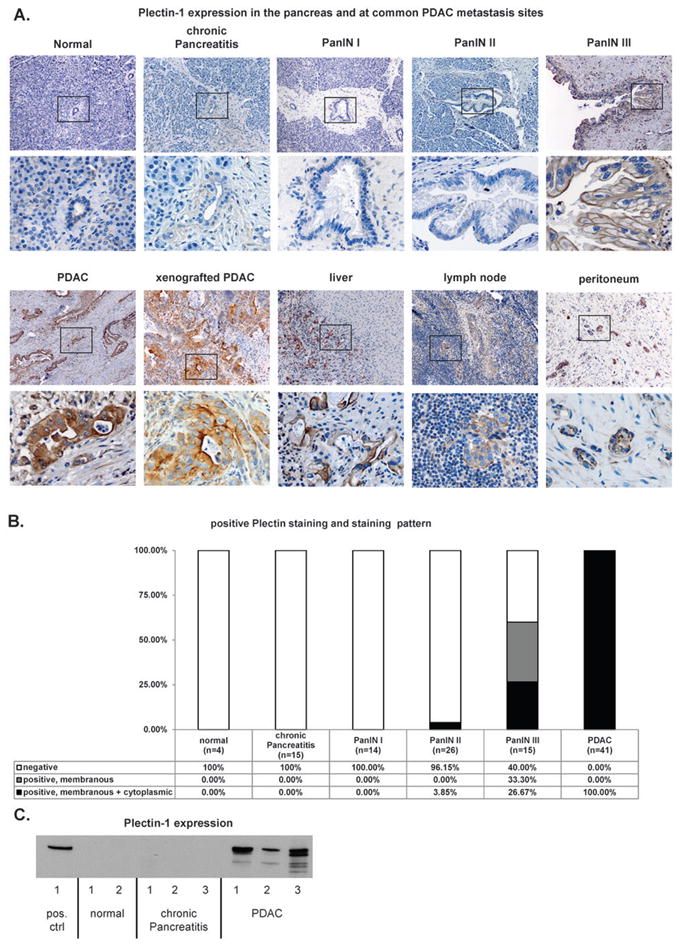
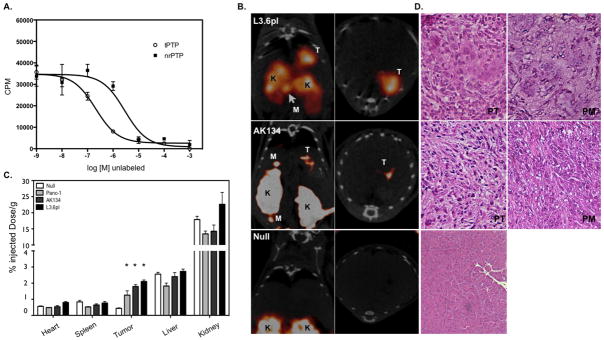
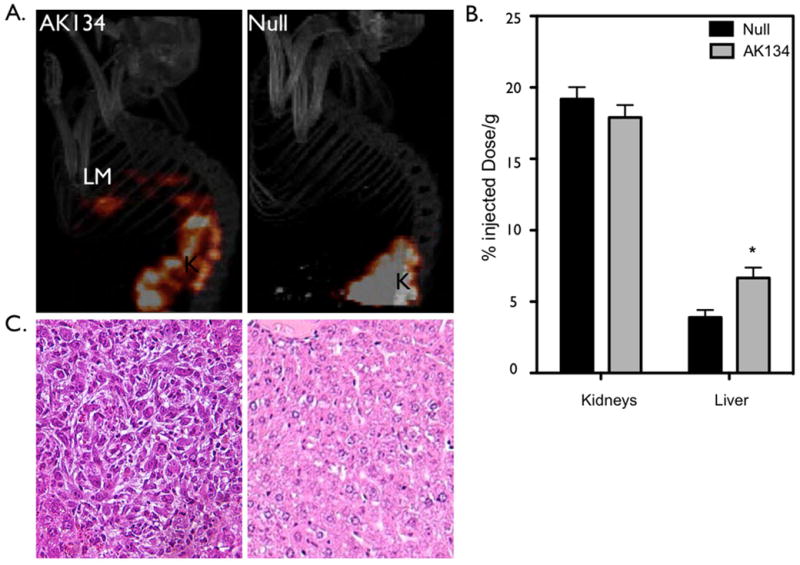
Experimental design: Specimens of human PDAC, chronic pancreatitis, and normal pancreata were evaluated by immunohistochemistry and Western blot analysis. To validate Plec1 as an imaging target, Plec1-targeting peptides (tPTP) were used as a contrast agent for single photon emission computed tomography in an orthotopic and liver metastasis murine model of PDAC.
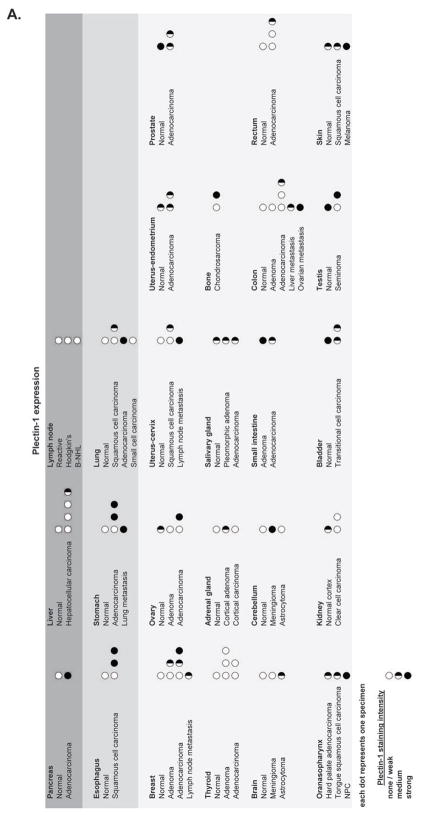
Results: Plec1 expression was noted to be positive in all PDACs but negative in benign tissues. Plec1 expression increases during pancreatic carcinogenesis. It was found to be misexpressed in only 0% to 3.85% of early PDAC precursor lesions (PanIN I/II) but in 60% of PanIN III lesions. Plec1 expression was further noted to be retained in all metastatic foci assayed and clearly highlighted these metastatic deposits in lymph nodes, liver, and peritoneum. In vivo imaging using tPTP specifically highlighted the primary and metastatic tumors. Biodistribution studies performed after imaging show that the primary pancreatic tumors and liver metastases retained 1.9- to 2.9-fold of tPTP over normal pancreas and 1.7-fold over normal liver.
Conclusions: Plec1 is the first biomarker to identify primary and metastatic PDAC by imaging and may also detect preinvasive PanIN III lesions. Strategies designed to image Plec1 could therefore improve detection and staging.
©2010 AACR.
Figures
Comment in
-
Blinded by the light: molecular imaging in pancreatic adenocarcinoma.Clin Cancer Res. 2011 Jan 15;17(2):203-5. doi: 10.1158/1078-0432.CCR-10-2825. Epub 2010 Nov 24. Clin Cancer Res. 2011. PMID: 21106729
References
-
- Jemal A, Siegel R, Ward E, Murray T, Xu J, Thun MJ. Cancer statistics, 2007. CA Cancer J Clin. 2007;57:43–66. - PubMed
-
- Furukawa H, Okada S, Saisho H, Ariyama J, Karasawa E, Nakaizumi A, et al. Clinicopathologic features of small pancreatic adenocarcinoma. A collective study. Cancer. 1996;78:986–90. - PubMed
-
- Krishna NB, Mehra M, Reddy AV, Agarwal B. EUS/EUS-FNA for suspected pancreatic cancer: influence of chronic pancreatitis and clinical presentation with or without obstructive jaundice on performance characteristics. Gastrointestinal Endoscopy. 2009;70:70–9. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
