

Dose-dense chemotherapy in nonmetastatic breast cancer: a systematic review and meta-analysis of randomized controlled trials
- PMID: 21098761
- PMCID: PMC3001963
- DOI: 10.1093/jnci/djq409
Dose-dense chemotherapy in nonmetastatic breast cancer: a systematic review and meta-analysis of randomized controlled trials
Abstract
Background: Dose-dense chemotherapy has become a mainstay regimen in the adjuvant setting for women with high-risk breast cancer. We performed a systematic review and meta-analysis of the existing data from randomized controlled trials regarding the efficacy and toxicity of the dose-dense chemotherapy approach in nonmetastatic breast cancer.
Methods: Randomized controlled trials that compared a dose-dense chemotherapy protocol with a standard chemotherapy schedule in the neoadjuvant or adjuvant setting in adult women older than 18 years with breast cancer were identified by searching The Cochrane Cancer Network register of trials, The Cochrane Library, and LILACS and MEDLINE databases (from January 1966 to January 2010). Hazard ratios (HRs) of death and recurrence and relative risks of adverse events were estimated and pooled. All statistical tests were two-sided.
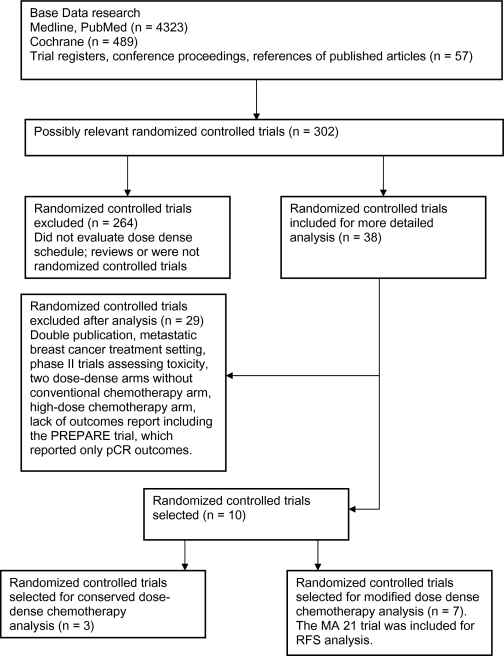
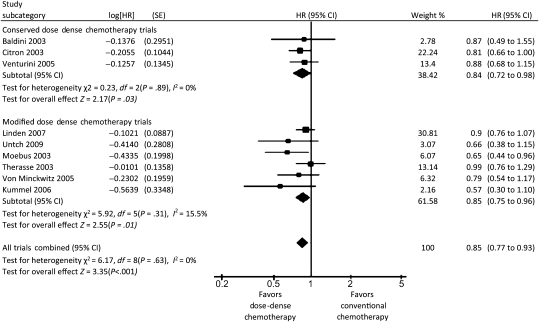
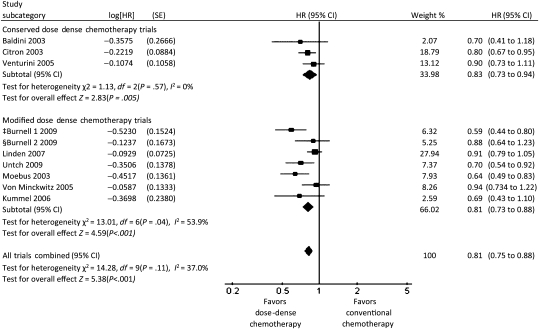
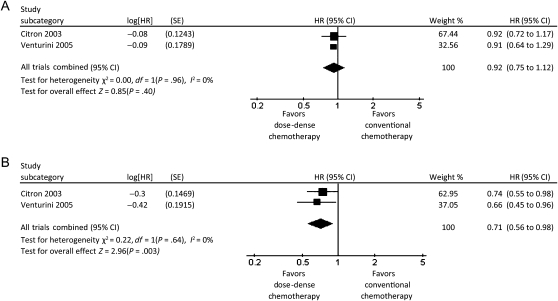
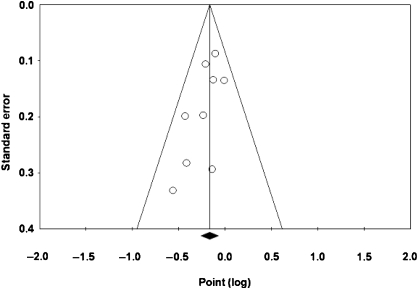
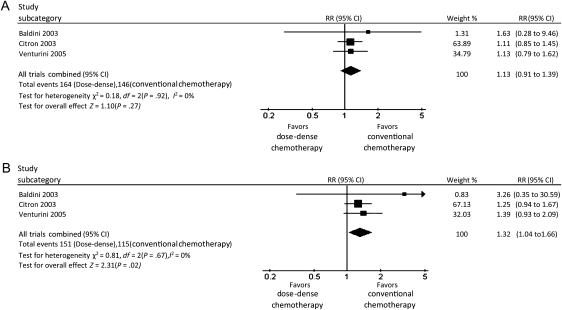
Results: Ten trials met the inclusion criteria and were classified into two categories based on trial methodology. Three trials enrolling 3337 patients compared dose-dense chemotherapy with a conventional chemotherapy schedule (similar agents). Patients who received dose-dense chemotherapy had better overall survival (HR of death = 0.84, 95% confidence interval [CI] = 0.72 to 0.98, P = .03) and better disease-free survival (HR of recurrence or death = 0.83, 95% CI = 0.73 to 0.94, P = .005) than those on the conventional schedule. No benefit was observed in patients with hormone receptor-positive tumors. Seven trials enrolling 8652 patients compared dose-dense chemotherapy with regimens that use standard intervals but with different agents and/or dosages in the treatment arms. Similar results were obtained for these trials with respect to overall survival (HR of death = 0.85, 95% CI = 0.75 to 0.96, P = .01) and disease-free survival (HR of recurrence or death = 0.81, 95% CI = 0.73 to 0.88, P < .001). The rate of nonhematological adverse events was higher in the dose-dense chemotherapy arms than in the conventional chemotherapy arms.
Conclusion: Dose-dense chemotherapy results in better overall and disease-free survival, particularly in women with hormone receptor-negative breast cancer. However, additional data from randomized controlled trials are needed before dose-dense chemotherapy can be considered as the standard of care.
Figures
Comment in
-
Meta-analysis: should it be more than the sum of its parts?J Natl Cancer Inst. 2010 Dec 15;102(24):1817-9. doi: 10.1093/jnci/djq469. Epub 2010 Nov 23. J Natl Cancer Inst. 2010. PMID: 21098760 No abstract available.
References
-
- Early Breast Cancer Trialists Collaborative Group (EBCTCG) Effects of chemotherapy and hormonal therapy for early breast cancer on recurrence and 15-year survival: an overview of the randomized trials. Lancet. 2005;365(9472):1687–1717. - PubMed
-
- Hryniuk WM. Average relative dose intensity and the impact on design of clinical trials. Semin Oncol. 1987;14(1):65. - PubMed
-
- Biganzoli L, Piccart MJ. The bigger the better? Or what we know and what we still need to learn about anthracycline dose per course, dose density and cumulative dose in the treatment of breast cancer. Ann Oncol. 1997;8(12):1177–1182. - PubMed
-
- Hudis C, Seidman A, Baselga J, et al. Sequential dose-dense doxorubicin, paclitaxel, and cyclophosphamide for resectable high-risk breast cancer: feasibility and efficacy. J Clin Oncol. 1999;17(1):93–100. - PubMed
-
- Norton La: A Gompertzian model of human breast cancer growth. Cancer Res. 1988;48(24, pt 1):7067. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
