

Case Reports
doi: 10.1159/000321791.
Epub 2010 Nov 24.
Plasma glial fibrillary acidic protein levels in a child with sickle cell disease and stroke
Affiliations
- PMID: 21099215
- PMCID: PMC3202928
- DOI: 10.1159/000321791
Item in Clipboard
Case Reports
Plasma glial fibrillary acidic protein levels in a child with sickle cell disease and stroke
Acta Haematol.
2011.
Abstract
A 12-year-old boy with HbSS sickle cell disease (SCD) was admitted with an acute febrile illness and developed overt stroke 3 days later. Plasma glial fibrillary acidic protein levels were elevated, as compared to pediatric controls, 32 h prior to the clinical diagnosis of stroke, peaked immediately prior to the exchange transfusion, and remained elevated 1 year later despite chronic transfusion therapy. Stroke in SCD can occur in the setting of acute illness, and a biomarker that could predict the onset and triage ill children to therapeutic intervention more quickly would be useful.
Copyright © 2010 S. Karger AG, Basel.
Figures
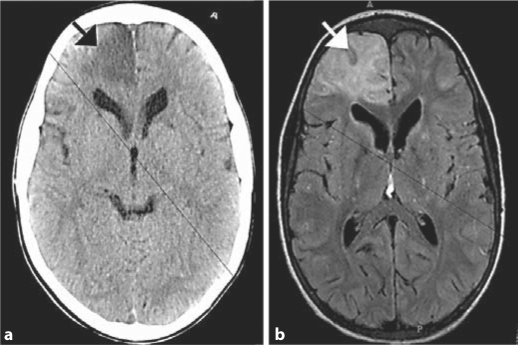
Neuroimaging of acute stroke in a 12-year-old HbSS patient who had plasma GFAP followed serially. a Noncontrast head CT immediately after clinical diagnosis of stroke showing a wedge of hypoattenuation in the right frontal lobe (arrow). b FLAIR MRI image 29 h after clinical diagnosis of stroke showing an evolving right anterior cerebral artery infarct (arrow).
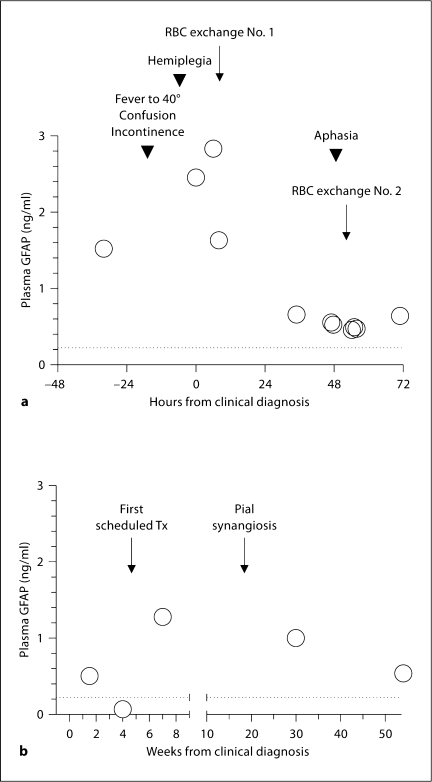
a Serial plasma GFAP levels in a 12-year-old patient with HbSS and acute stroke. A red cell exchange transfusion was performed 5 h after clinical diagnosis and again 47 h later for new neurologic deficits. The dotted line marks the 95th percentile value among 60 healthy pediatric controls. Arrowheads mark the presentation of relevant signs and symptoms. b Fifty-four weeks of follow-up GFAP measurements.
Similar articles
-
Plasma glial fibrillary acidic protein levels in children with sickle cell disease.Am J Hematol. 2011 May;86(5):427-9. doi: 10.1002/ajh.21995. Am J Hematol. 2011. PMID: 21523806 Free PMC article. Clinical Trial.
-
Effect of Chronic Blood Transfusion on Biomarkers of Coagulation Activation and Thrombin Generation in Sickle Cell Patients at Risk for Stroke.PLoS One. 2015 Aug 25;10(8):e0134193. doi: 10.1371/journal.pone.0134193. eCollection 2015. PLoS One. 2015. PMID: 26305570 Free PMC article. Clinical Trial.
-
Brain-derived neurotrophic factor levels in pediatric sickle cell disease.Pediatr Blood Cancer. 2020 Feb;67(2):e28076. doi: 10.1002/pbc.28076. Epub 2019 Nov 17. Pediatr Blood Cancer. 2020. PMID: 31736231 Free PMC article.
-
Role of glial fibrillary acidic protein as a biomarker in differentiating intracerebral haemorrhage from ischaemic stroke and stroke mimics: a meta-analysis.Biomarkers. 2020 Feb;25(1):1-8. doi: 10.1080/1354750X.2019.1691657. Epub 2019 Nov 28. Biomarkers. 2020. PMID: 31702405
-
Glial fibrillary acidic protein for the early diagnosis of intracerebral hemorrhage: Systematic review and meta-analysis of diagnostic test accuracy.Int J Stroke. 2019 Jun;14(4):390-399. doi: 10.1177/1747493018806167. Epub 2018 Oct 10. Int J Stroke. 2019. PMID: 30303809
Cited by
-
Targeting novel mechanisms of pain in sickle cell disease.Hematology Am Soc Hematol Educ Program. 2017 Dec 8;2017(1):546-555. doi: 10.1182/asheducation-2017.1.546. Hematology Am Soc Hematol Educ Program. 2017. PMID: 29222304 Free PMC article. Review.
-
Neuroprotective, anti-inflammatory, and analgesic activity of palmitoylethanolamide in sickle cell mice.Blood Adv. 2025 Jun 24;9(12):3056-3068. doi: 10.1182/bloodadvances.2024015439. Blood Adv. 2025. PMID: 40085960 Free PMC article.
-
Rewarming Rate During Cardiopulmonary Bypass Is Associated With Release of Glial Fibrillary Acidic Protein.Ann Thorac Surg. 2015 Oct;100(4):1353-8. doi: 10.1016/j.athoracsur.2015.04.006. Epub 2015 Jul 7. Ann Thorac Surg. 2015. PMID: 26163357 Free PMC article.
-
GFAP and Neuron Specific Enolase (NSE) in the Serum of Suicide Attempters.Med J Islam Repub Iran. 2022 Sep 7;36:103. doi: 10.47176/mjiri.36.103. eCollection 2022. Med J Islam Repub Iran. 2022. PMID: 36447551 Free PMC article.
-
Evidence of an association between brain cellular injury and cognitive decline after non-cardiac surgery.Br J Anaesth. 2016 Jan;116(1):83-9. doi: 10.1093/bja/aev415. Br J Anaesth. 2016. PMID: 26675953 Free PMC article.
References
-
- Ohene-Frempong K, Weiner SJ, Sleeper LA, Miller ST, Embury S, Moohr JW, Wethers DL, Pegelow CH, Gill FM. Cerebrovascular accidents in sickle cell disease: rates and risk factors. Blood. 1998;91:288–294. - PubMed
-
- Verduzco LA, Nathan DG. Sickle cell disease and stroke. Blood. 2009;114:5117–5125. - PubMed
-
- Adams RJ, Brambilla D. Discontinuing prophylactic transfusions used to prevent stroke in sickle cell disease. N Engl J Med. 2005;353:2769–2778. - PubMed
-
- Woertgen C, Rothoerl RD, Wiesmann M, Missler U, Brawanski A. Glial and neuronal serum markers after controlled cortical impact injury in the rat. Acta Neurochir Suppl. 2002;81:205–207. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
