

Review
doi: 10.4161/isl.2.5.13019.
Epub 2010 Sep 1.
Surgical aspects of human islet isolation
Affiliations
- PMID: 21099323
- PMCID: PMC3230558
- DOI: 10.4161/isl.2.5.13019
Item in Clipboard
Review
Surgical aspects of human islet isolation
Islets.
2010 Sep-Oct.
Abstract
Islet transplantation is a safe and effective procedure; however, it depends on the critical step of isolating high quality of islets from whole pancreas. Human islet isolation requires considerable experience and expertise, and is frequently seen as 'an art rather than a science'. However, without scientific knowledge of pancreatic anatomy, real experience can not be gained. In particular, an understanding ductal anatomy is important to perform human islet isolation. This review is based on clinical experience of more than 900 human islet isolations performed over 10 years and aims to highlight pancreatic anatomy and surgical techniques in islet processing.
Figures
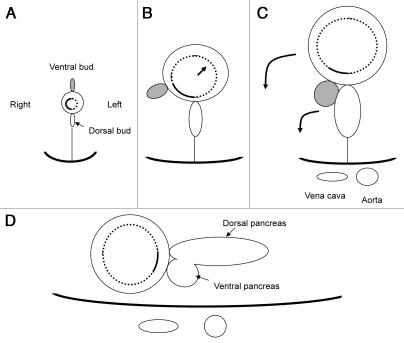
Hypothetical schema showing ‘rotation’ of duodenum and pancreas (transverse section). (A) A ventral pancreatic bud appears in the ventral wall of the primitive duodenum. (B) As a result of expansion of the left side of the duodenum, the ventral pancreas passively comes to the right. (C) The ventral pancreas fuses with the dorsal pancreas. (D) Final retroperitoneal position of duodenum and pancreas.
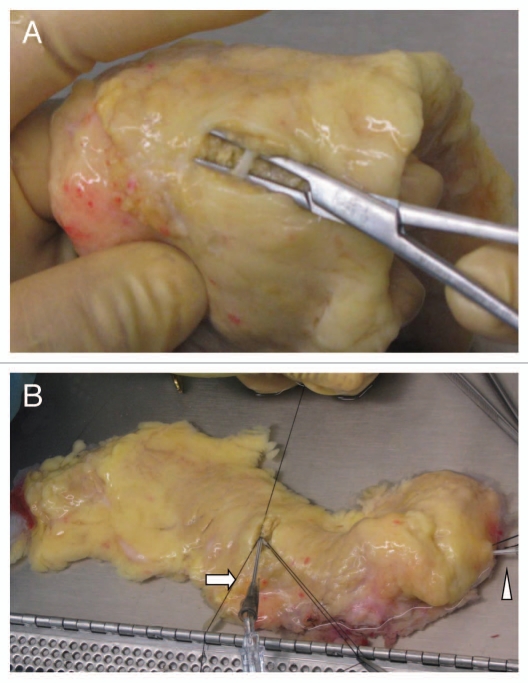
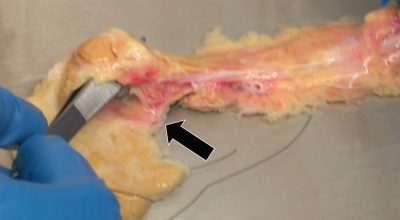
A catheter insertion at the mid-body. (A) The main pancreatic duct is exposed at the mid-body. (B) A 16 gauge catheter is inserted into the main duct toward the tail (arrow). Arrowhead points to a catheter inserted into the main duct from the head.
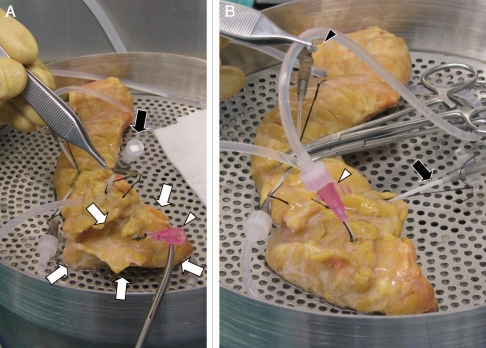
Intraductal distention in case of complete type of pancreas divisum. (A) The dorsal pancreas is being distended using two catheters inserted at the mid-body. The ventral pancreas (white arrows) is not distended. There is no fluid emptying from a small catheter (20 gauge) inserted into the orifice of Wirsung duct (white arrowhead), indicating no ductal communications between the ventral and dorsal systems. (B) The ventral pancreas is being distended through the Wirsung duct (white arrowhead). There is no fluid emptying from a catheter at the mid-body (black arrowhead), again indicating no ductal communications between the ventral and dorsal systems. Black arrow indicates a catheter inserted into the orifice of Santorini duct.
In this case, the duodenal diverticulum was not recognized from the outside appearance of the pancreas and duodenum.
Appearance of the duodenum after dissection of the pancreas. Arrows indicate an area around the minor duodenal papilla where the pancreatic tissue was invading to the duodenal wall.
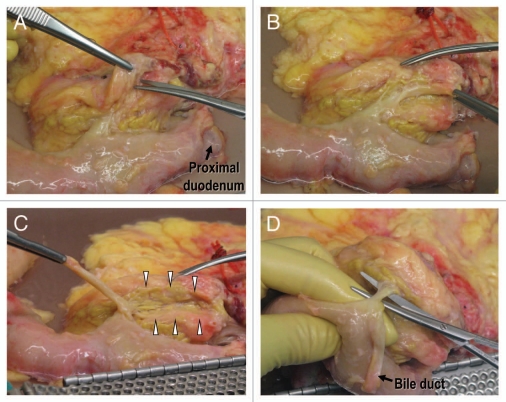
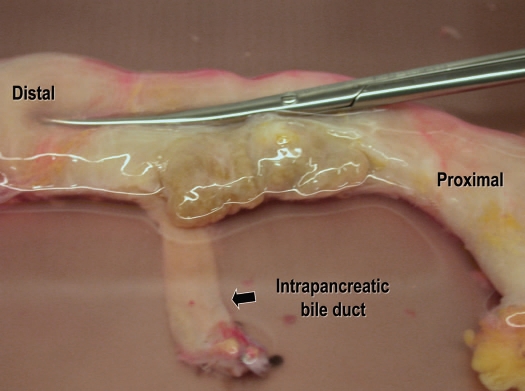
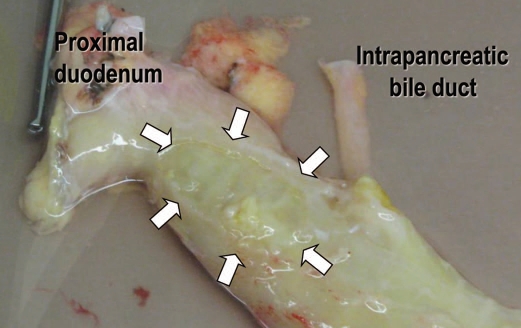
Posterior aspect of the pancreatoduodenal region. (A) There is a fusion cleft to the right of the intrapancreatic bile duct. (B) The intrapancreatic bile duct is exposed in its entire length without any injury to the pancreatic parenchyma. (C) The intrapancreatic bile duct is retracted by the forceps. Groove for passage of the bile duct can be seen (arrowheads). (D) The main pancreatic duct is exposed.
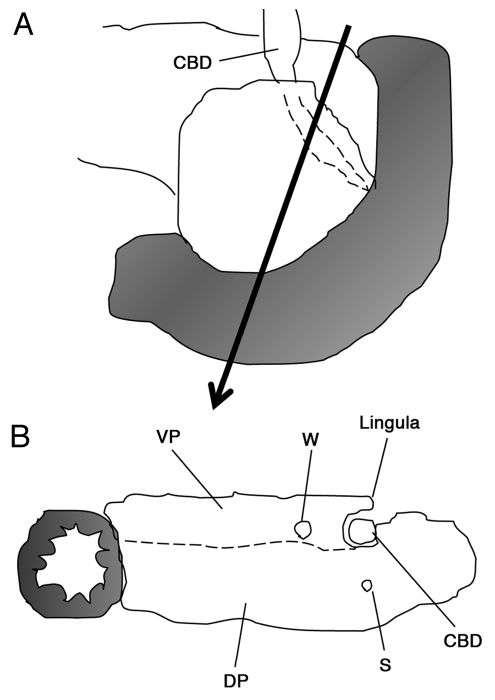
Schema showing the pancreatic lingula. (A) Posterior aspect of the pancreatoduodenal region. (B) The intrapanceratic bile duct is covered by the pancreatic lingula. The lingula is derived from the ventral pancreas. A dotted line indicates a border between the ventral and dorsal pancreata, however, such a border can not be identified macroscopically. CBD, common bile duct; VP, ventral pancreas; DP, dorsal pancreas; W, Wirsung duct; S, Santorini duct.
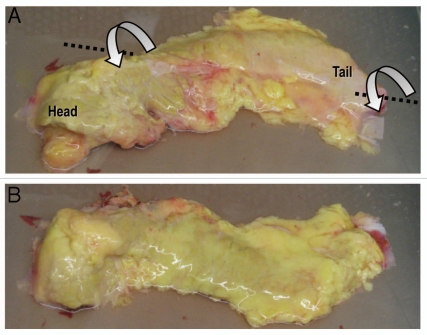
(A) The posterior aspect of the body/tail is facing the observer while the head portion is placed in anatomical position. Note a smooth surface transition from the head to body. (B) The body/tail is being twisted on its long axis by 180° anterior-inferiorly. The whole pancreas is now placed in anatomical position.

Annular pancreas. Forceps are inserted to show the passage of the duodenum.
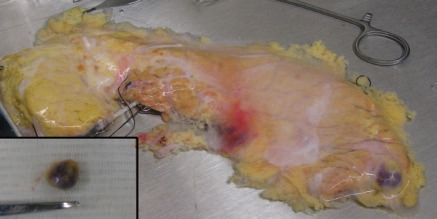
An accessory spleen embedded into the tail of the pancreas. Inset: the accessory spleen was extirpated after intraductal distention of the pancreas.
Circumportal pancreas. The uncinate process is communicating with the posterior aspect of the pancreas body (arrow). Forceps are inserted to show the passage of the portal vein.

Posterior view of congenital short pancreas. Inset: a length of catheter is shown.

Heavily fat infiltrated pancreas. The parenchyma of the pancreas is hardly seen from the surface.
References
-
- Shapiro AM, Lakey JR, Ryan EA, Korbutt GS, Toth E, Warnock GL, et al. Islet transplantation in seven patients with type 1 diabetes mellitus using a glucocorticoid-free immunosuppressive regimen. N Engl J Med. 2000;343:230–238. - PubMed
-
- Ryan EA, Paty BW, Senior PA, Bigam D, Alfadli E, Kneteman NM, et al. Five-year follow-up after clinical islet transplantation. Diabetes. 2005;54:2060–2069. - PubMed
-
- Gruessner RWG, Sutherland DER, Kandaswamy R, Gruessner AC. Over 500 solitary pancreas transplants in nonuremic patients with brittle diabetes mellitus. Transplantation. 2008;85:42–47. - PubMed
-
- Bellin M, Barton F, Hering B the investigators of the Collaborative Islet Transplant Registry, author. Induction immunosuppression with T-cell depleting antibodies facilitates longterm insulin independence after islet allotransplantation in type 1 diabetes. Xenotransplantation. 2009;16:541.
-
- Danovitch GM, Cohen DJ, Weir MR, Stock PG, Bennett WM, Christensen LL, et al. Current status of kidney and pancreas transplantation in the United States 1994–2003. Am J Transplant. 2005;5:904–915. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources