

Elevation of blood urea nitrogen is predictive of long-term mortality in critically ill patients independent of "normal" creatinine
- PMID: 21099426
- PMCID: PMC3448784
- DOI: 10.1097/CCM.0b013e3181ffe22a
Elevation of blood urea nitrogen is predictive of long-term mortality in critically ill patients independent of "normal" creatinine
Abstract
Objective: We hypothesized that elevated blood urea nitrogen can be associated with all-cause mortality independent of creatinine in a heterogeneous critically ill population.
Design: Multicenter observational study of patients treated in medical and surgical intensive care units.
Setting: Twenty intensive care units in two teaching hospitals in Boston, MA.
Patients: A total of 26,288 patients, age ≥ 18 yrs, hospitalized between 1997 and 2007 with creatinine of 0.80-1.30 mg/dL.
Interventions: None.
Measurements: Blood urea nitrogen at intensive care unit admission was categorized as 10-20, 20-40, and >40 mg/dL. Logistic regression examined death at days 30, 90, and 365 after intensive care unit admission as well as in-hospital mortality. Adjusted odds ratios were estimated by multivariable logistic regression models.
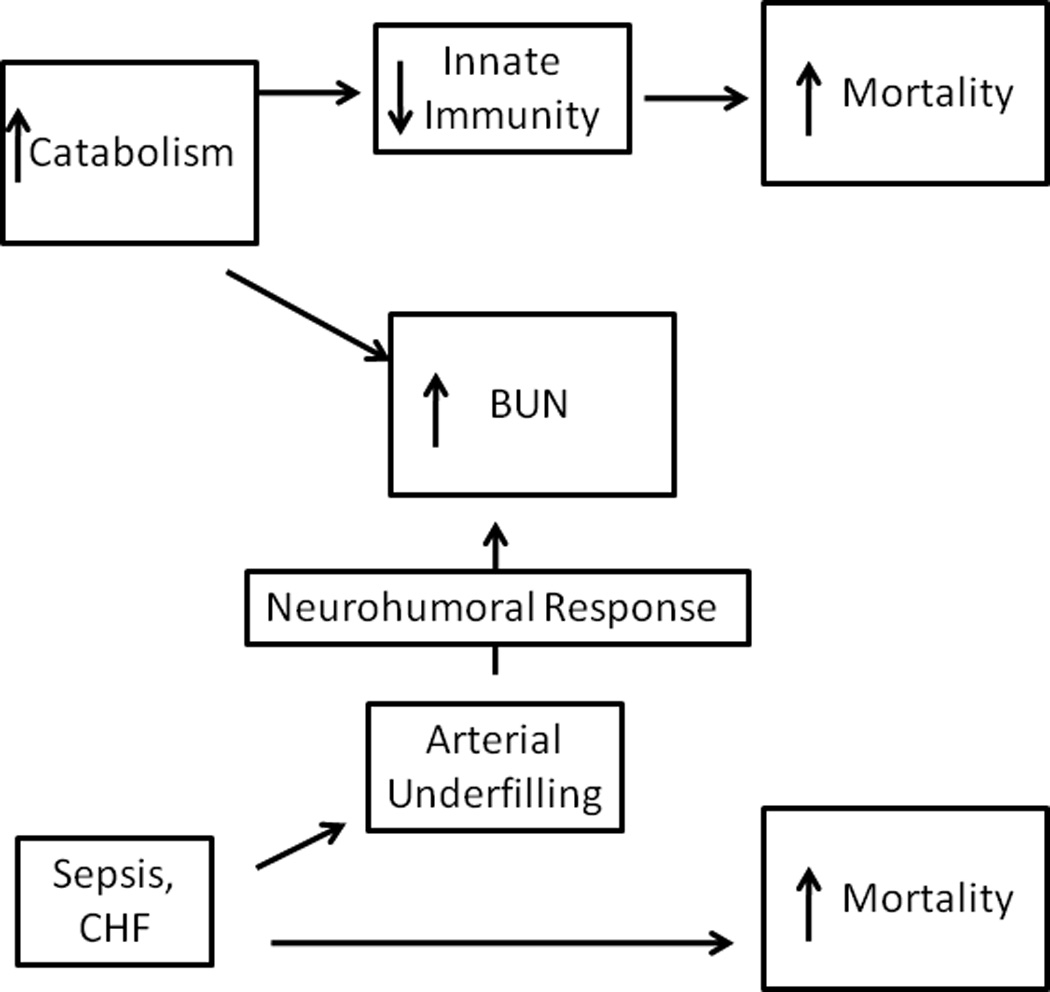
Main results: Blood urea nitrogen at intensive care unit admission was predictive for short- and long-term mortality independent of creatinine. Thirty days following intensive care unit admission, patients with blood urea nitrogen of >40 mg/dL had an odds ratio for mortality of 5.12 (95% confidence interval, 4.30-6.09; p < .0001) relative to patients with blood urea nitrogen of 10-20 mg/dL. Blood urea nitrogen remained a significant predictor of mortality at 30 days after intensive care unit admission following multivariable adjustment for confounders; patients with blood urea nitrogen of >40 mg/dL had an odds ratio for mortality of 2.78 (95% confidence interval, 2.27-3.39; p < .0001) relative to patients with blood urea nitrogen of 10-20 mg/dL. Thirty days following intensive care unit admission, patients with blood urea nitrogen of 20-40 mg/dL had an odds ratio of 2.15 (95% confidence interval, 1.98-2.33; <.0001) and a multivariable odds ratio of 1.53 (95% confidence interval, 1.40-1.68; p < .0001) relative to patients with blood urea nitrogen of 10-20 mg/dL. Results were similar at 90 and 365 days following intensive care unit admission as well as for in-hospital mortality. A subanalysis of patients with blood cultures (n = 7,482) demonstrated that blood urea nitrogen at intensive care unit admission was associated with the risk of blood culture positivity.
Conclusion: Among critically ill patients with creatinine of 0.8-1.3 mg/dL, an elevated blood urea nitrogen was associated with increased mortality, independent of serum creatinine.
Conflict of interest statement
The authors have no potential conflicts of interest to disclose.
Figures
Comment in
-
Blood urea nitrogen beyond estimation of renal function.Crit Care Med. 2011 Feb;39(2):405-6. doi: 10.1097/CCM.0b013e318205c33a. Crit Care Med. 2011. PMID: 21248523 No abstract available.
References
-
- Johnson WJ, Hagge WW, Wagoner RD, et al. Effects of urea loading in patients with far-advanced renal failure. Mayo Clin Proc. 1972;47:21–29. - PubMed
-
- Meyer TW, Hostetter TH. Uremia. N Engl J Med. 2007;357:1316–1325. - PubMed
-
- Hartz AJ, Kuhn EM, Kayser KL, et al. BUN as a risk factor for mortality after coronary artery bypass grafting. Ann Thorac Surg. 1995;60:398–404. - PubMed
-
- Felker GM, Leimberger JD, Califf RM, et al. Risk stratification after hospitalization for decompensated heart failure. J Card Fail. 2004;10:460–466. - PubMed
-
- Fonarow GC, Adams KF, Jr, Abraham WT, et al. Risk stratification for in-hospital mortality in acutely decompensated heart failure: classification and regression tree analysis. Jama. 2005;293:572–580. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
