

Neonatal outcomes after demonstrated fetal lung maturity before 39 weeks of gestation
- PMID: 21099593
- PMCID: PMC4074509
- DOI: 10.1097/AOG.0b013e3181fb7ece
Neonatal outcomes after demonstrated fetal lung maturity before 39 weeks of gestation
Abstract
Objective: To compare outcomes among neonates delivered after documentation of fetal lung maturity before 39 weeks and those delivered at 39 or 40 weeks.
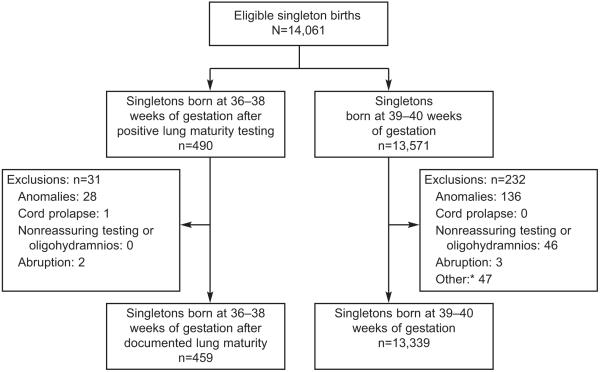
Methods: This was a retrospective cohort study of women with singleton pregnancy delivered at 36 0/7 to 38 6/7 weeks after positive fetal lung maturity testing (based on amniotic fluid lecithin to sphingomyelin ratio) or at 39 0/7 to 40 6/7 weeks (without maturity testing) at our center from 1999 to 2008. Women with fetuses with major congenital anomalies, cord prolapse, nonreassuring antepartum testing, placental abruption, or oligohydramnios were excluded. A primary composite neonatal outcome included death, adverse respiratory outcomes, hypoglycemia, treated hyperbilirubinemia, generalized seizures, necrotizing enterocolitis, hypoxic ischemic encephalopathy, periventricular leukomalacia, and suspected or proven sepsis.
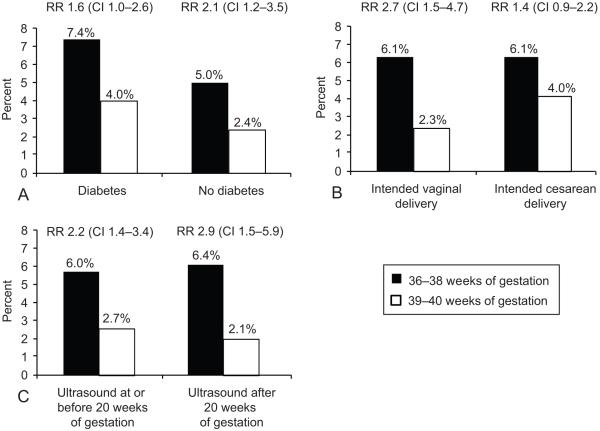
Results: There were 459 neonates delivered at 36 to 38 weeks and 13,339 delivered at 39 to 40 weeks; mean birth weight was 3,107±548 g and 3,362±439 g, respectively. The risk of the composite adverse neonatal outcome was 6.1% for the 36- to 38-week group compared with 2.5% for the 39- to 40-week group (relative risk 2.4; confidence interval [CI] 1.7-3.5). After multivariable adjustment, early delivery remained significantly associated with an increased risk of the composite outcome (adjusted odds ratio [OR]1.7; CI 1.1-2.6) as well as several individual outcomes, including respiratory distress syndrome (adjusted OR 7.6; CI 2.2-26.6), treated hyperbilirubinemia (adjusted OR 11.2; CI 3.6-34), and hypoglycemia (adjusted OR 5.8; CI 2.4-14.3).
Conclusion: Neonates delivered at 36 to 38 weeks after confirmed fetal lung maturity are at higher risk of adverse outcomes than those delivered at 39 to 40 weeks.
Figures

Comment in
-
Neonatal outcomes after demonstrated fetal lung maturity before 39 weeks of gestation.Obstet Gynecol. 2011 May;117(5):1228-1229. doi: 10.1097/AOG.0b013e3182175dbf. Obstet Gynecol. 2011. PMID: 21508772 No abstract available.
References
-
- Morrison JJ, Rennie JM, Milton PJ. Neonatal respiratory morbidity and mode of delivery at term: influence of timing of elective cesarean section. Br J Obstet Gynaecol. 1995;102:101–6. - PubMed
-
- Zanardo V, Simbi AK, Franzoi M, Solda G, Salvadori A, Trevisanuto D. Neonatal respiratory morbidity risk and mode of delivery at term: influence of timing of elective cesarean delivery. Acta Paediatr. 2004;93:643–7. - PubMed
-
- Tita AT, Landon MB, Spong CY, Lai Y, Leveno KJ, Varner MW, Moawad AH, Caritis SN, Meis PJ, Wapner RJ, Sorokin Y, Miodovnik M, Carpenter M, Peaceman AM, O’Sullivan MJ, Sibai BM, Langer O, Thorp JM, Ramin SM, Mercer BM. Eunice Kennedy Shriver NICHD Maternal-Fetal Medicine Units Network. Timing of elective repeat cesarean delivery at term and neonatal outcomes. N Engl J Med. 2009;360:111–20. - PMC - PubMed
-
- American College of Obstetricians and Gynecologists . Fetal maturity assessment prior to elective repeat cesarean delivery. ACOG Committee Opinion Number 98. ACOG; Washington, DC: 1991.
-
- American College of Obstetricians and Gynecologists Cesarean delivery on maternal request. ACOG Committee Opinion Number 394. Obstet Gynecol. 2007;110:1501–4. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
