

Rate of and risks for regression of cervical intraepithelial neoplasia 2 in adolescents and young women
- PMID: 21099605
- PMCID: PMC3057366
- DOI: 10.1097/AOG.0b013e3181fe777f
Rate of and risks for regression of cervical intraepithelial neoplasia 2 in adolescents and young women
Abstract
Objective: To describe the natural history of cervical intraepithelial neoplasia (CIN) 2 in a prospective study of adolescents and young women, and to examine the behavioral and biologic factors associated with regression and progression.
Methods: Adolescents and women aged 13 to 24 years who were referred for abnormal cytology and were found to have CIN 2 on histology were evaluated at 4-month intervals. Risks for regression were defined as three consecutive negative cytology and histology visits, and progression to CIN 3 was estimated using Cox proportional hazards regression models.
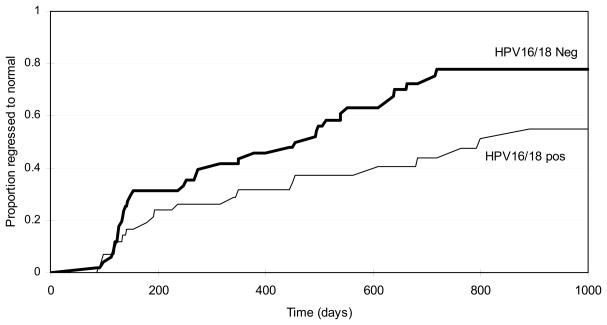
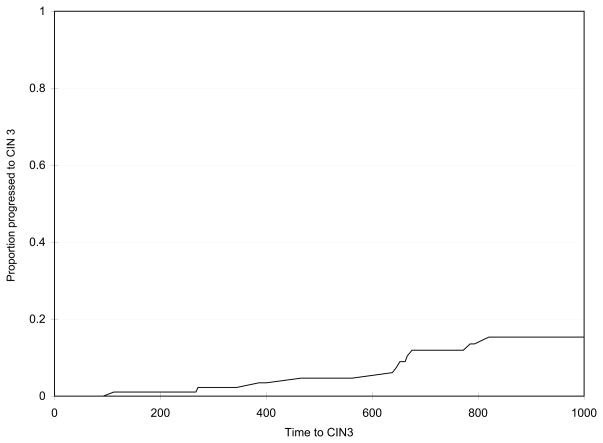
Results: Ninety-five patients with a mean age of 20.4 years (±2.3) were entered into the analysis. Thirty-eight percent resolved by year 1, 63% resolved by year 2, and 68% resolved by year 3. Multivariable analysis found that recent Neisseria gonorrhoeae infection (hazard ratio 25.27; 95% confidence interval [CI] 3.11-205.42) and medroxyprogesterone acetate use (per month) (hazard ratio 1.02; 95% CI 1.003-1.04) were associated with regression. Factors associated with nonregression included combined hormonal contraception use (per month) (hazard ratio 0.85; 95% CI 0.75-0.97) and persistence of human papillomavirus (HPV) of any type (hazard ratio 0.40; 95% CI 0.22-0.72). Fifteen percent of patients showed progression by year 3. HPV 16/18 persistence (hazard ratio 25.27; 95% CI 2.65-241.2; P=.005) and HPV 16/18 status at last visit (hazard ratio 7.25; 95% CI 1.07-49.36; P<.05) were associated with progression Because of the small sample size, other covariates were not examined.
Conclusion: The high regression rate of CIN 2 supports clinical observation of this lesion in adolescents and young women.
Figures


References
-
- Cox JT, Schiffman M, Solomon D ASCUS-LSIL Triage Study (ALTS) Group. Prospective follow-up suggests similar risk of subsequent cervical intraepithelial neoplasia grade 2 or 3 among women with cervical intraepithelial neoplasia grade 1 or negative colposcopy and directed biopsy. Am J Obstet Gynecol. 2003;188(6):1406–12. - PubMed
-
- Nassiel K, Nassiel M, Vaclavinkova V. Behavior of Moderate Cervical Dysplasia During Long Term Follow-Up. 1983;61(5):609–14. - PubMed
-
- Syrjanen K, Kataja V, Yliskoski M, Chang F, Syrjanen S. Natural History of Cervical Human Papillomavirus Lesions Does Not Substantiate the Biologic Relevance of the Bethesda System. 1992;79(5 Pt 1):675–82. - PubMed
-
- Moscicki AB, Shiboski S, Hills NK, Powell KJ, Jay N, Hanson EN, et al. Regression of low-grade squamous intra-epithelial lesions in young women. Lancet. 2004;364(9446):1678–83. - PubMed
-
- Wright TC, Jr, Massad LS, Dunton CJ, Spitzer M, Wilkinson EJ, Solomon D. 2006 consensus guidelines for the management of women with cervical intraepithelial neoplasia or adenocarcinoma in situ. Am J Obstet Gynecol. 2007 Oct;197(4):340–5. - PubMed
