

Sequelae of Perthes disease: treatment with surgical hip dislocation and relative femoral neck lengthening
- PMID: 21102198
- PMCID: PMC3031125
- DOI: 10.1097/BPO.0b013e3181fcbaaf
Sequelae of Perthes disease: treatment with surgical hip dislocation and relative femoral neck lengthening
Abstract
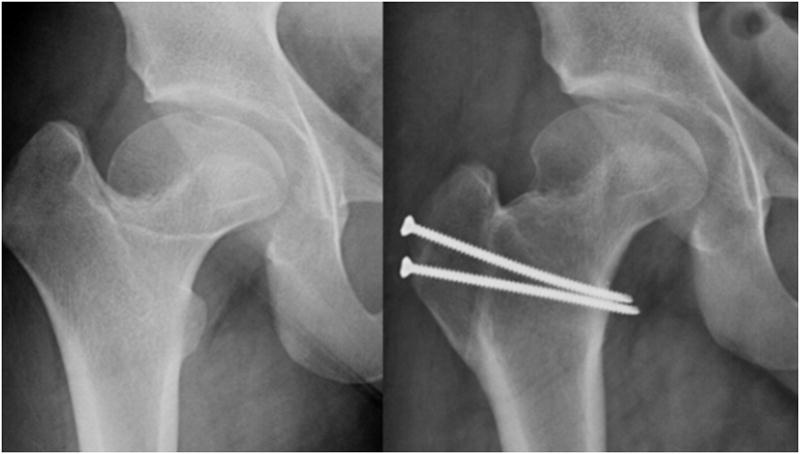
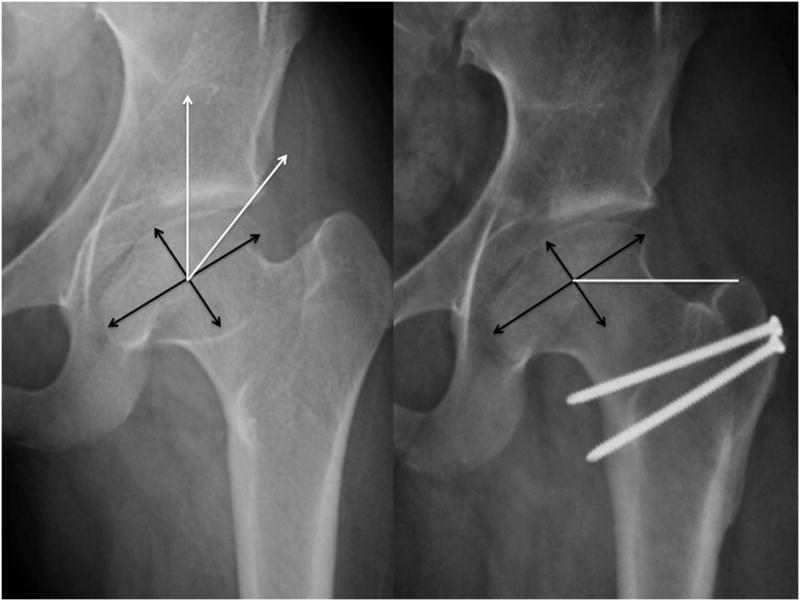
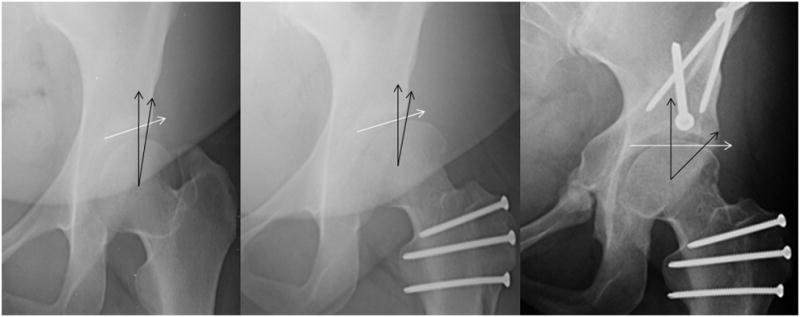
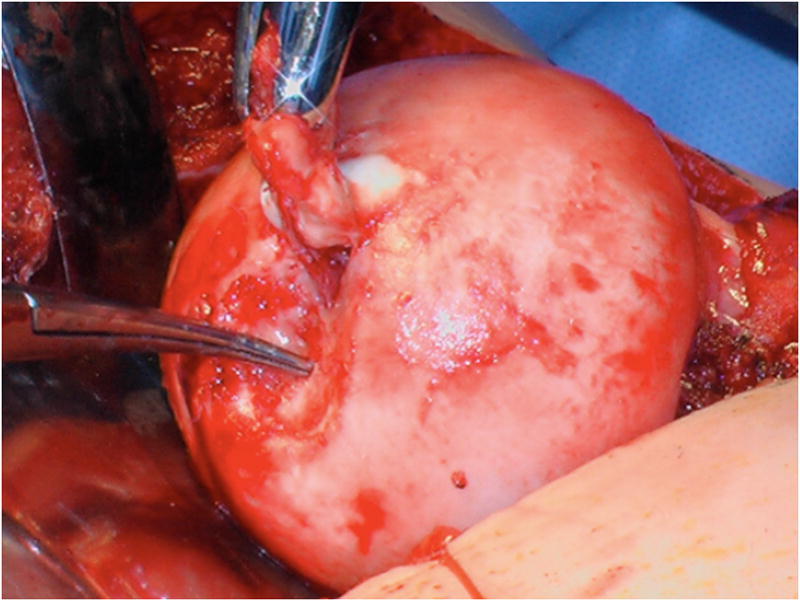
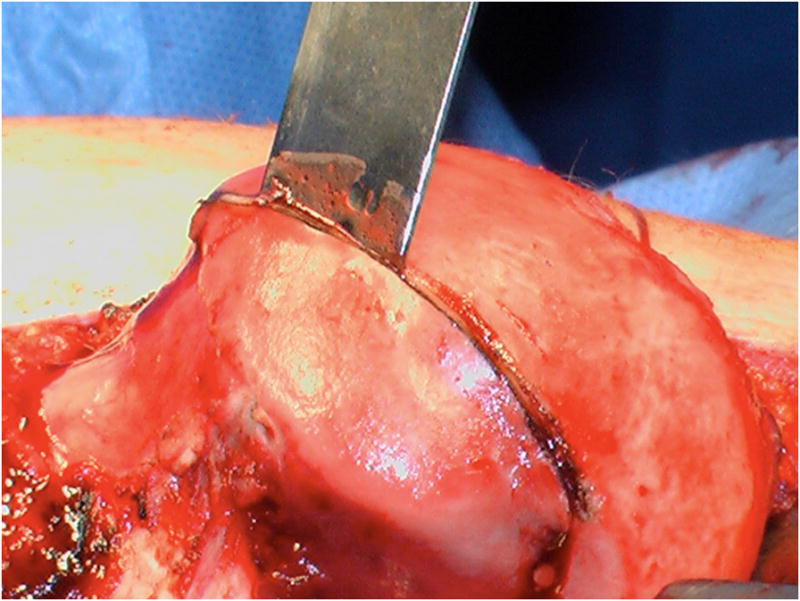
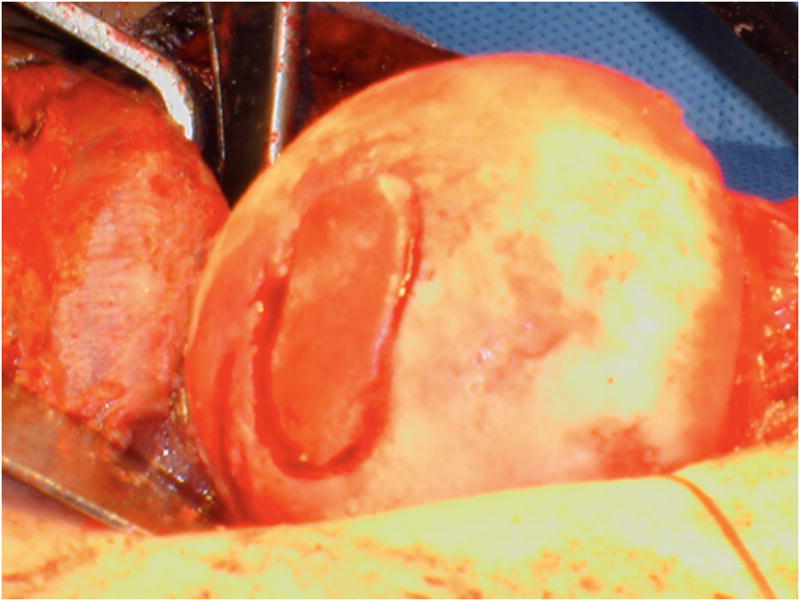
Background: Sequelae of Perthes disease commonly manifests as complex hip pathomorphology including coxa magna, coxa brevis, and acetabular dysplasia. These abnormalities contribute to femoroacetabular impingement and early osteoarthritis. This report describes our experience with correction of the proximal femoral deformity associated with Perthes disease through surgical dislocation, osteochondroplasty (SDO), trochanteric advancement, and treatment of intraarticular chondrolabral injury.
Methods: Between January 2003 and January 2009, 14 patients with Perthes disease (4 female and 10 male patients) with an average age of 19.6 years (range 14 to 28 y) were treated with SDO and trochanteric advancement. One patient had a subsequent staged periacetabular osteotomy to improve acetabular coverage. Patient histories, physical examinations, operative findings, and preoperative and postoperative radiographs were evaluated.
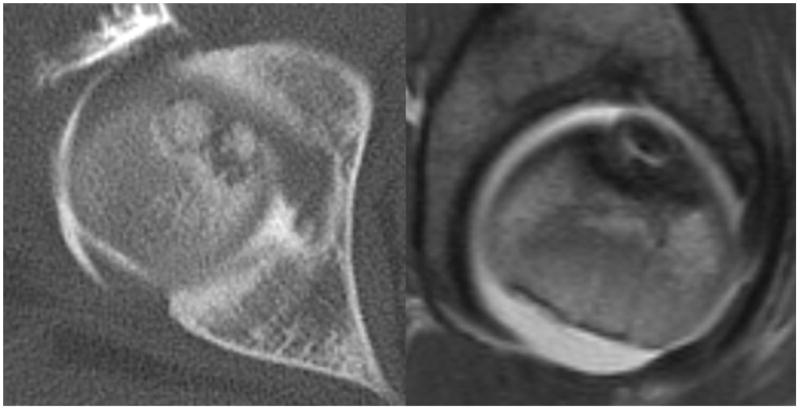
Results: Operative findings showed 6 acetabular cartilage lesions, 6 labral lesions, and 4 femoral osteochondritis dissecans (OCD) lesions treated with autografts. The mean of center-trochanteric distance improved from -20 mm to -1 mm. Approximately 4 of 14 hips deteriorated to Tönnis grade 1 and 1 of 14 hips deteriorated 2 Tönnis grades. The Harris hip scores improved from an average of 62 preoperatively (range 51 to 72) to 95 postoperatively (range 93 to 97) with OCD lesions versus 71 (range 65 to 76) to 88.6 (range 63 to 100) in the hips without OCD lesions. There was no statistically significant difference in the age, preoperative or postoperative HHSs between the OCD and non-OCD groups. The mean follow-up was 45 months. There were no major perioperative complications, and all the patients in both the groups have their native hip to date.
Conclusions: The typical adult sequelae of Perthes disease predispose the hip to the development of chondrolabral injury and poor clinical function. Treatment with SDO and trochanteric advancement reduces impingement, improves hip biomechanics, and allows the treatment of intraarticular pathology. This approach is associated with clinical improvement without major perioperative complications. In addition, we have found a high rate of OCD lesions of the femoral head in Perthes hips undergoing surgical dislocation. Osteochondral autograft transfer from the resected femoral head-neck junction been found in the 4 patients treated thus far to be safe and effective with comparable clinical and radiographic outcomes to those hips without OCD lesions.
Level of evidence: Level IV (Case series).
Figures


References
-
- Wenger DR, Kishan S, Pring ME. Impingement and childhood hip disease. J Pediatr Orthop B. 2006;15:233–243. - PubMed
-
- Amstutz HC, Antoniades JT, Le Duff MJ. Results of metal-on-metal hybrid hip resurfacing for Crowe type-I and II developmental dysplasia. J Bone Joint Surg Am. 2007;89:339–346. - PubMed
-
- Boyd HS, Ulrich SD, Seyler TM, Marulanda GA, Mont MA. Resurfacing for Perthes disease: an alternative to standard hip arthroplasty. Clinical orthopaedics and related research. 2007;465:80–85. - PubMed
-
- Clohisy JC, Keeney JA, Schoenecker PL. Preliminary assessment and treatment guidelines for hip disorders in young adults. Clinical orthopaedics and related research. 2005;441:168–179. - PubMed
-
- Ganz R, Gill TJ, Gautier E, Ganz K, Krugel N, Berlemann U. Surgical dislocation of the adult hip a technique with full access to the femoral head and acetabulum without the risk of avascular necrosis. The Journal of bone and joint surgery. 2001;83:1119–1124. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
