

Visible iris sign as a predictor of problems during and following anterior approach ptosis surgery
- PMID: 21102489
- PMCID: PMC3169219
- DOI: 10.1038/eye.2010.177
Visible iris sign as a predictor of problems during and following anterior approach ptosis surgery
Abstract
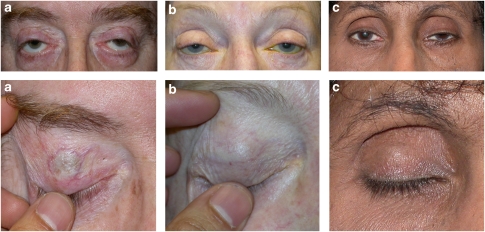
Objective: To describe the pre- and postoperative features of the visible iris sign (VIS), which is the apparent visibility of iris colour through a closed upper eyelid, in patients undergoing anterior approach surgery for severe involutional aponeurotic ptosis, and to assess its effect on postoperative outcome.
Design: Prospective, comparative interventional case series.
Methods: Prospective series of all patients undergoing surgery for severe involutional aponeurotic ptosis during a 16-month period at a single centre.
Inclusion criteria: Severe involutional ptosis (upper eyelid margin reflex distance (MRD) ≤1 mm) treated by anterior-approach surgery.
Main outcome measures: Presence of VIS, type of ptosis (primary or recurrent), preoperative MRD, levator function and skin crease height, documented unusual intra-operative findings, postoperative complications, and follow-up time.
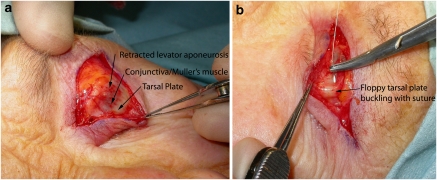
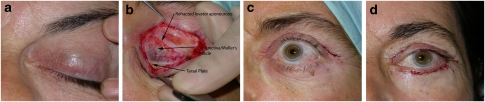
Results: Of 133 procedures for involutional aponeurotic ptosis, 96 procedures (56 patients) were included in the study. In total, 12 patients (21%, 12/56, 2 males, and 10 females) had been identified as having VIS preoperatively. In order to avoid any selection bias, only patients with severe degree of ptosis were included in the two groups with the two groups being alike in the preoperative lid height, levator function or the skin crease. In the VIS group, 55% (12/22) had a thinned, significantly retracted levator aponeurosis and a thin tarsus prone to full-thickness suture passes (36.3%, 8/22) during aponeurosis reattachment. Immediate persistent overcorrection during surgery was seen in three procedures, with one patient having an under corrected outcome when treated with a hang-back suture. In the non-VIS group, no patients were documented intra-operatively, as having significant retraction of the levator aponeurosis. However, 14% (10/74) of the eyelids were recorded as having a very attenuated levator and one patient (3%, 1/44) was noted to have a floppy tarsus that was difficult to suture. The total incidence of intra-operative difficulties during surgery were 78% in the VIS group and 22% in the non-VIS group. Mean postoperative follow-up was 22 weeks. (median 18, range 12-64). The overall success rates were 63.6% (14/22) in the VIS group, compared with 77.0% (57/74) in the non-VIS group (P = 0.260). After excluding cases undergoing concurrent blepharoplasty and non-Caucasians, success rates were 57.1% (4/7) and 69.2% (9/13) in the VIS and non-VIS groups, respectively (P = 0.598). All failures were because of under-correction.
Conclusion: The VIS is a clinical sign of severe involutional ptosis. Patients with VIS have one or more features, including a retracted levator aponeurosis, a thinned tarsus prone to full-thickness suture passes, and a tendency for immediate persistent overcorrection following levator advancement. Preoperative identification of VIS may help in appropriate patient counselling, procedure selection, anticipation of intraoperative difficulties, and possibly further standardisation of future cohorts when evaluating the results of involutional ptosis surgery. PRÉCIS: The authors describe the pre-, intra- and postoperative features of visible iris sign. They discuss the success rates of anterior approach surgery in VIS patients and discuss the contributing factors for a poorer outcome.
Figures
References
-
- Leatherbarrow B.BlepharoptosisIn: Martin Dunitz (ed).Oculoplastic Surgery Taylor and Francis: London; 200221–43.
-
- Siddens DJ, Nesi FA.Aquired ptosis: classification and evaluationNesi F, Lisman R, Levine R (eds). Smith's Ophthalmic Plastic and reconstructive surgery Mosby -Year Book Inc: St Louis; 1998380–381.
-
- Martin P, Rogers P. Involutional ptosis: recognition and management. Aust NZ J Ophthalmol. 1985;13 (2:185–187. - PubMed
-
- Collin J. Involutional ptosis. Aust NZ J Ophthalmol. 1986;14:109–112. - PubMed
-
- Holstrom H, Fillip C. Aponeurotic repair of involutional blepharoptosis. Scand J Plast Reconstr Surg Hand Surg. 2002;36:160–165. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
