

Unusual Development of Iatrogenic Complex, Mixed Biliary and Duodenal Fistulas Complicating Roux-en-Y Antrectomy for Stenotic Peptic Disease of the Supraampullary Duodenum Requiring Whipple Procedure: An Uncommon Clinical Dilemma
- PMID: 21103208
- PMCID: PMC2988862
- DOI: 10.1159/000322027
Unusual Development of Iatrogenic Complex, Mixed Biliary and Duodenal Fistulas Complicating Roux-en-Y Antrectomy for Stenotic Peptic Disease of the Supraampullary Duodenum Requiring Whipple Procedure: An Uncommon Clinical Dilemma
Abstract
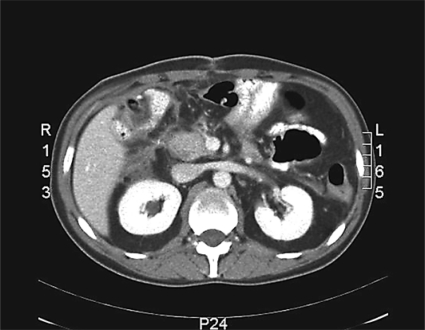
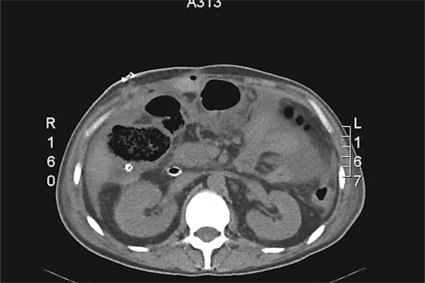
Complex fistulas of the duodenum and biliary tree are severe complications of gastric surgery. The association of duodenal and major biliary fistulas occurs rarely and is a major challenge for treatment. They may occur during virtually any kind of operation, but they are more frequent in cases complicated by the presence of difficult duodenal ulcers or cancer, with a mortality rate of up to 35%. Options for treatment are many and range from simple drainage to extended resections and difficult reconstructions. Conservative treatment is the choice for well-drained fistulas, but some cases require reoperation. Very little is known about reoperation techniques and technical selection of the right patients. We present the case of a complex iatrogenic duodenal and biliary fistula. A 42-year-old Caucasian man with a diagnosis of postoperative peritonitis had been operated on 3 days earlier; an antrectomy with a Roux-en-Y reconstruction for stenotic peptic disease was performed. Conservative treatment was attempted with mixed results. Two more operations were required to achieve a definitive resolution of the fistula and related local complications. The decision was made to perform a pancreatoduodenectomy with subsequent reconstruction on a double jejunal loop. The patient did well and was discharged on postoperative day 17. In our experience pancreaticoduodenectomy may be an effective treatment of refractory and complex iatrogenic fistulas involving both the duodenum and the biliary tree.
Figures

Similar articles
-
Laparoscopic Pancreas-Sparing Duodenectomy with Roux en Y Reconstruction for Duodenal Polyposis.Chirurgia (Bucur). 2019 Jul-Aug;114(4):494-505. doi: 10.21614/chirurgia.114.4.502. Chirurgia (Bucur). 2019. PMID: 31511136
-
Two cases of a perforated duodenal diverticulum after gastrectomy with Roux-en-Y reconstruction.Surg Case Rep. 2019 Nov 5;5(1):169. doi: 10.1186/s40792-019-0738-y. Surg Case Rep. 2019. PMID: 31691035 Free PMC article.
-
Management of gastrogastric fistulas after divided Roux-en-Y gastric bypass surgery for morbid obesity: analysis of 1,292 consecutive patients and review of literature.Surg Obes Relat Dis. 2005 Sep-Oct;1(5):467-74. doi: 10.1016/j.soard.2005.07.003. Epub 2005 Aug 31. Surg Obes Relat Dis. 2005. PMID: 16925272 Review.
-
Postoperative duodenal fistulas. A report of 23 cases with emphasis on the surgical treatment by the Roux-en-Y operation.Acta Chir Belg. 1985 May-Jun;85(3):185-91. Acta Chir Belg. 1985. PMID: 3929511
-
Hybrid laparoscopic-robotic management of type IVa choledochal cyst in the setting of prior Roux-en-Y gastric bypass: video case report and review of the literature.Surg Endosc. 2015 Jun;29(6):1648-54. doi: 10.1007/s00464-014-3937-4. Epub 2014 Dec 10. Surg Endosc. 2015. PMID: 25492448 Review.
Cited by
-
Iatrogenic Non-Reconstructable Duodenal Injury Presenting without Peritonitis: An Indication of Pancreatoduodenectomy in the Presence of Safe Hands. A Case Report.Cureus. 2017 Apr 6;9(4):e1138. doi: 10.7759/cureus.1138. Cureus. 2017. PMID: 28484677 Free PMC article.
References
-
- Dudrick SJ, Maharaj AR, McKelvey AA. Artificial nutritional support in patients with gastrointestinal fistulas. World J Surg. 1999;23:570–576. - PubMed
-
- Agarwal N, Sharma BC, Garg S, Kumar R, Sarin SK. Endoscopic management of postoperative bile leaks. Hepatobiliary Pancreat Dis Int. 2006;5:273–277. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
