

Case Reports
doi: 10.1159/000254613.
Endoscopic Biliary Drainage Using Guidewire Cannulation in a Case with Severe Duodenal Stenosis Caused by Duodenal Undifferentiated Carcinoma
Affiliations
- PMID: 21103223
- PMCID: PMC2988893
- DOI: 10.1159/000254613
Item in Clipboard
Case Reports
Endoscopic Biliary Drainage Using Guidewire Cannulation in a Case with Severe Duodenal Stenosis Caused by Duodenal Undifferentiated Carcinoma
Case Rep Gastroenterol.
.
Abstract
We present a case of duodenal carcinoma, 12 cm in size, with severe stenosis at the second portion of the duodenum. When the patient developed obstructive jaundice, it was impossible to perform endoscopic biliary drainage by standard cannulation due to the stenosis, but was succeeded by wire-guided cannulation using papillotome. Histology of the tumor showed undifferentiated carcinoma without differentiation to any specific cell type. Systemic chemotherapy was started with 5-FU, leucovorin and oxaliplatin. Biliary stent worked well until the patient succumbed three months after. Herein we demonstrate the new advantage of wire-guided cannulation in case of duodenal stenosis.
Figures
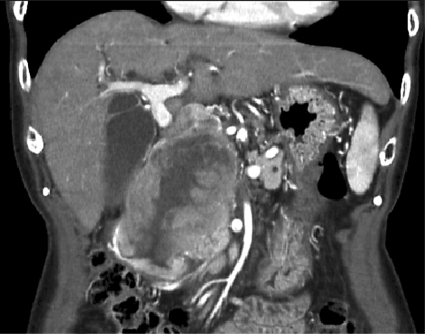
Abdominal CT showing a bulky tumor located at the second portion of the duodenum, 12 cm in largest diameter.
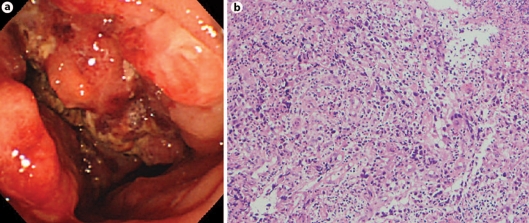
a Endoscopic view of the duodenum showing a large tumor with ulceration and necrosis, and with duodenal stenosis at the second portion. b Histology of forceps biopsy from the tumor demonstrates undifferentiated carcinoma with abundant inflammatory cell infiltration (×100, hematoxylin and eosin).
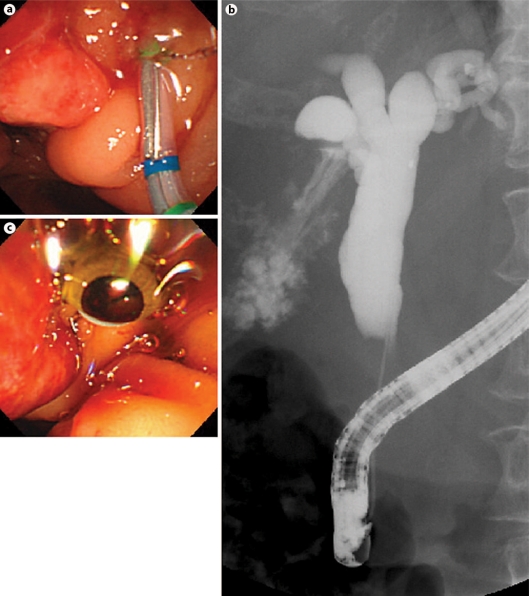
Guidewire cannulation using papillotome (a), following deep cannulation to the bile duct (b) and biliary stent insertion (c).
Similar articles
-
Utility of Endoscopic Ultrasound-Guided Hepaticogastrostomy with Antegrade Stenting for Malignant Biliary Obstruction after Failed Endoscopic Retrograde Cholangiopancreatography.Oncology. 2017;93 Suppl 1:69-75. doi: 10.1159/000481233. Epub 2017 Dec 20. Oncology. 2017. PMID: 29258066
-
Temporary placement of a covered duodenal stent can avoid riskier anterograde biliary drainage when ERCP for obstructive jaundice fails due to duodenal invasion.Surg Endosc. 2017 Feb;31(2):625-631. doi: 10.1007/s00464-016-5008-5. Epub 2016 Jun 20. Surg Endosc. 2017. PMID: 27324333
-
Combined duodenal stent placement and endoscopic ultrasonography-guided biliary drainage for malignant duodenal obstruction with biliary stricture.Dig Endosc. 2010 Jul;22(3):236-40. doi: 10.1111/j.1443-1661.2010.00997.x. Dig Endosc. 2010. PMID: 20642617
-
Biliary therapy: are we ready for EUS-guidance?Minerva Med. 2007 Aug;98(4):379-84. Minerva Med. 2007. PMID: 17921954 Review.
-
Selective biliary cannulation techniques for endoscopic retrograde cholangiopancreatography procedures and prevention of post- endoscopic retrograde cholangiopancreatography pancreatitis.Expert Rev Gastroenterol Hepatol. 2016 Jun;10(6):709-22. doi: 10.1586/17474124.2016.1143774. Epub 2016 Feb 6. Expert Rev Gastroenterol Hepatol. 2016. PMID: 26782710 Review.
References
-
- Freeman ML, Guda NM. ERCP cannulation: a review of reported techniques. Gastrointest Endosc. 2005;61:112–125. - PubMed
-
- Schwacha H, Allgaier HP, Deibert P, Olschewski M, Allgaier U, Blum HE. A sphincterotome-based technique for selective transpapillary common bile duct cannulation. Gastrointest Endosc. 2000;52:387–391. - PubMed
-
- Cortas GA, Mehta SN, Abraham NS, Barkun AN. Selective cannulation of the common bile duct: a prospective randomized trial comparing standard catheters with sphincterotomes. Gastrointest Endosc. 1999;50:775–779. - PubMed
-
- Maindrault-Goebel F, de Gramont A, Louvet C, et al. Evaluation of oxaliplatin dose intensity in bimonthly leucovorin and 48-hour 5-fluorouracil continuous infusion regimens (FOLFOX) in pretreated metastatic colorectal cancer. Oncology Multidisciplinary Research Group (GERCOR) Ann Oncol. 2000;11:1477–1483. - PubMed
-
- Yamao K, Bhatia V, Mizuno N, et al. EUS-guided choledochoduodenostomy for palliative biliary drainage in patients with malignant biliary obstruction: results of long-term follow-up. Endoscopy. 2008;40:340–342. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
