

Radiofrequency ablation of hepatocellular carcinoma: pros and cons
- PMID: 21103289
- PMCID: PMC2989542
- DOI: 10.5009/gnl.2010.4.S1.S113
Radiofrequency ablation of hepatocellular carcinoma: pros and cons
Abstract
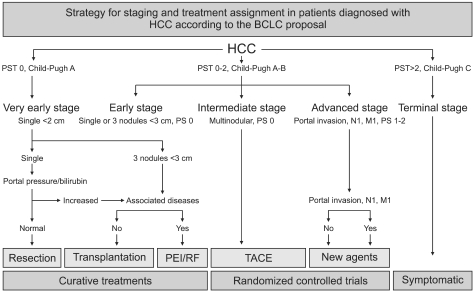
Among locoregional treatments for hepatocellular carcinoma (HCC), radiofrequency ablation (RFA) has been accepted as the most popular alternative to curative transplantation or resection, and it shows an excellent local tumor control rate and acceptable morbidity. The benefits of RFA have been universally validated by the practice guidelines of international societies of hepatology. The main advantages of RFA include 1) it is minimally invasive with acceptable morbidity, 2) it enables excellent local tumor control, 3) it has promising long-term survival, and 4) it is a multimodal approach. Based on these pros, RFA will play an important role in managing the patient with early HCC (smaller than 3 cm with fewer than four tumors). The main limitations of current RFA technology in hepatic ablation include 1) limitation of ablation volume, 2) technically infeasible in some tumors due to conspicuity and dangerous location, and 3) the heat-sink effect. Many technical approaches have been introduced to overcome those limitations, including a novel guiding modality, use of artificial fluid or air, and combined treatment strategies. RFA will continue to play a role as a representative ablative modality in the management of HCC, even in the era of targeted agents.
Keywords: Hepatocellular carcinoma; Image-guided tumor ablation; Loco-regional therapy; Radiofrequency ablation; Thermal ablation.
Figures
References
-
- Bosch FX, Ribes J, Cleries R, Diaz M. Epidemiology of hepatocellular carcinoma. Clin Liver Dis. 2005;9:191–211. - PubMed
-
- Stuart KE, Anand AJ, Jenkins RL. Hepatocellular carcinoma in the United States. Prognostic features, treatment outcome, and survival. Cancer. 1996;77:2217–2222. - PubMed
-
- Bruix J, Sherman M. Management of hepatocellular carcinoma. Hepatology. 2005;42:1208–1236. - PubMed
-
- Hong K, Georgiades CS, Geschwind JF. Technology insight: Image-guided therapies for hepatocellular carcinoma--intra-arterial and ablative techniques. Nat Clin Pract Oncol. 2006;3:315–324. - PubMed
-
- Jansen MC, van Hillegersberg R, Chamuleau RA, van Delden OM, Gouma DJ, van Gulik TM. Outcome of regional and local ablative therapies for hepatocellular carcinoma: a collective review. Eur J Surg Oncol. 2005;31:331–347. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
