

EUS-Guided Biliary Drainage
- PMID: 21103298
- PMCID: PMC2989556
- DOI: 10.5009/gnl.2010.4.S1.S67
EUS-Guided Biliary Drainage
Abstract
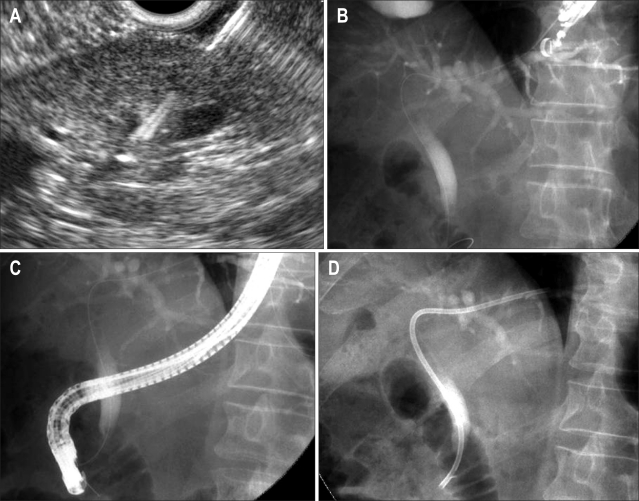
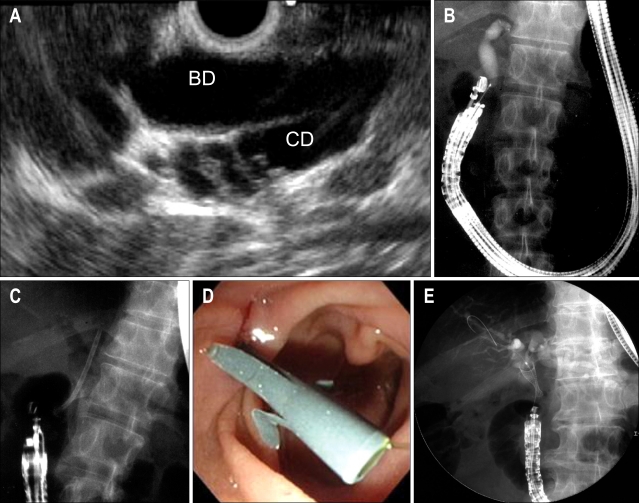
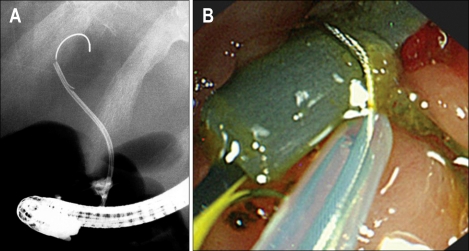
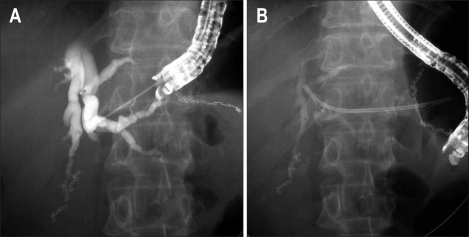
Endoscopic ultrasonography (EUS) combines endoscopy and intraluminal ultrasonography, and allows imaging with a high-frequency transducer over a short distance to generate high-resolution ultrasonographic images. EUS is now a widely accepted modality for diagnosing pancreatobiliary diseases. EUS-guided fine-needle aspiration (EUS-FNA) using a curved linear-array echoendoscope was initially described more than 20 years ago, and since then many researchers have expanded its indications to sample diverse lesions and have also used it for various therapeutic purposes. EUS-guided biliary drainage (EUS-BD) is one of the therapeutic procedures that has been developed using a curved linear-array echoendoscope. Technically, EUS-BD includes rendezvous techniques via transesophageal, transgastric, and transduodenal routes, EUS-guided choledochoduodenostomy (EUS-CDS), and EUS-guided hepaticogastrostomy (EUS-HGS). Published data have demonstrated a high success rate, albeit with a comparatively high rate of nonfatal complications for EUS-CDS and EUS-HGS, and a comparatively low success rate with a low complication rate for the rendezvous technique. At present, these procedures represent an alternative to surgery or percutaneous transhepatic biliary drainage (PTBD) for patients with obstructive jaundice when endoscopic biliary drainage (EBD) has failed. However, these procedures should be performed in centers with extensive experience in linear EUS and therapeutic biliary ERCP. Large prospective studies are needed in the near future to establish standardized EUS-BD procedures as well as to perform controlled comparative trials between EUS-BD and PTBD, between rendezvous techniques and direct-access techniques (EUS-CDS and EUS-HGS), and between EBD and EUS-BD.
Keywords: Endoscopic ultrasonography; Endoscopic ultrasonography-guided biliary drainage; Endoscopic ultrasonography-guided choledochoduodenostomy; Endoscopic ultrasonography-guided hepaticogastrostomy; Rendezvous technique.
Figures
References
-
- Vilmann P, Jacobsen GK, Henriksen FW, Hancke S. Endoscopic ultrasonography with guided fine needle aspiration biopsy in pancreatic disease. Gastrointest Endosc. 1992;38:172–173. - PubMed
-
- Bhutani MS. Endoscopic ultrasound guided fine needle aspiration of pancreas. In: Bhutani MS, editor. Interventional Endoscopic Ultrasonography. Amsterdam: Harwood Academic; 1999. pp. 65–72.
-
- Wiersema MJ, Sandusky D, Carr R, Wiersema LM, Erdel WC, Frederick PK. Endosonography-guided cholangiopancreatography. Gastrointest Endosc. 1996;43:102–106. - PubMed
-
- Giovannini M, Moutardier V, Pesenti C, Bories E, Lelong B, Delpero JR. Endoscopic ultrasound-guided bilioduodenal anastomosis: a new technique for biliary drainage. Endoscopy. 2001;33:898–900. - PubMed
-
- Burmester E, Niehaus J, Leineweber T, Huetteroth T. EUS-cholangio-drainage of the bile duct: report of 4 cases. Gastrointest Endosc. 2003;57:246–251. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
