

Left-sided appendicitis: review of 95 published cases and a case report
- PMID: 21105193
- PMCID: PMC2992678
- DOI: 10.3748/wjg.v16.i44.5598
Left-sided appendicitis: review of 95 published cases and a case report
Abstract
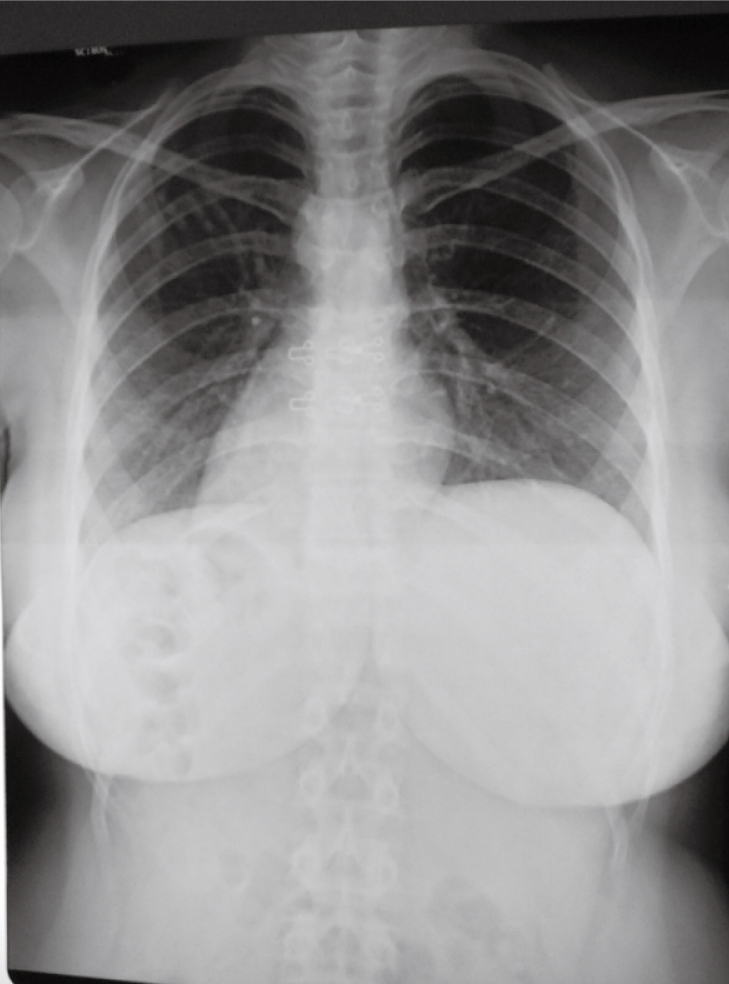
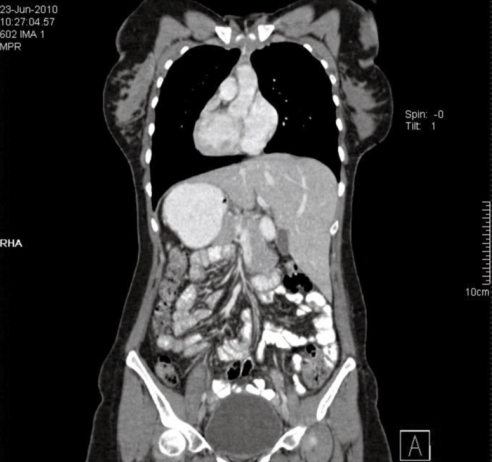
Aim: To give an overview of the literature on left-sided acute appendicitis (LSAA) associated with situs inversus totalis (SIT) and midgut malrotation (MM).
Methods: We present a new case of LSAA with SIT and a literature review of studies published in the English language on LSAA, accessed via PubMed and Google Scholar databases.
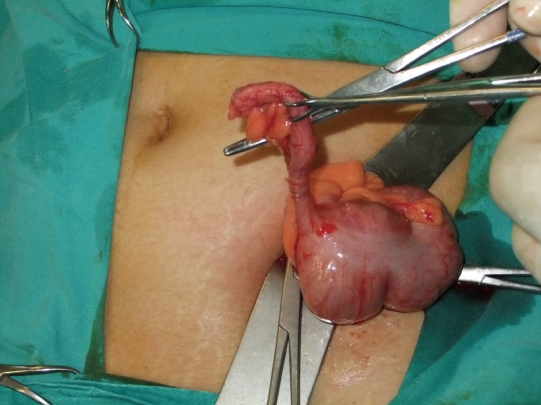
Results: Ninety-five published cases of LSAA were evaluated and a 25-year-old female, who presented to our clinic with left lower abdominal pain caused by LSAA, is reported. In the reviewed literature, fifty-seven patients were male and 38 were female with an age range of 8 to 82 years and a median age of 29.1 ± 15.9 years. Sixty-six patients had SIT, 23 had MM, three had cecal malrotation, and two had a previously unnoted congenital abnormality. Fifty-nine patients had presented to the hospital with left lower, 14 with right lower and seven with bilateral lower quadrant pain, and seven subjects complained of left upper quadrant pain. The diagnosis was established preoperatively in 49 patients, intraoperatively in 19, and during the postoperative period in five; 14 patients were aware of having this anomaly. The data of eight patients were not unavailable. Eleven patients underwent laparoscopic appendectomy, which was combined with cholecystectomy in two cases. Histopathological examination of the appendix specimens revealed adenocarcinoma in only two of 95 patients.
Conclusion: The diagnosis of left lower quadrant pain is based on well-established clinical symptoms, physical examination and physician's experience.
Figures
References
-
- Akbulut S, Caliskan A, Ekin A, Yagmur Y. Left-sided acute appendicitis with situs inversus totalis: review of 63 published cases and report of two cases. J Gastrointest Surg. 2010;14:1422–1428. - PubMed
-
- Hou SK, Chern CH, How CK, Kao WF, Chen JD, Wang LM, Huang CI. Diagnosis of appendicitis with left lower quadrant pain. J Chin Med Assoc. 2005;68:599–603. - PubMed
-
- Franklin ME Jr, Almeida JA, Pérez ER, Michaelson RLP, Majarrez A. Cholecystectomy and appendectomy by laparoscopy in a patient with situs inversus totalis: A case report and review of the literature. Asoc Mex Cir Endoscopica. 2001;2:150–153.
-
- van Steensel CJ, Wereldsma JC. Acute appendicitis in complete situs inversus. Neth J Surg. 1985;37:117–118. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
